By John Leake
Courageous Discourse
December 9, 2024
Many viewers of the surveillance footage of the murder of Brian Thompson perceived the assassin to be using a semi-automatic pistol and to have experienced multiple cartridge jams that required him to cycle the bolt manually. More likely he used a non-auto-ejecting, single-shot bolt action pistol. The advantage of this design is that it drives all of the combustion down the barrel and into the integrated silencer instead of bleeding gas off to cycle the bolt, which is considerably louder.
In other words, the assassin apparently favored silence over speed, and the weapon he chose may have been the following.
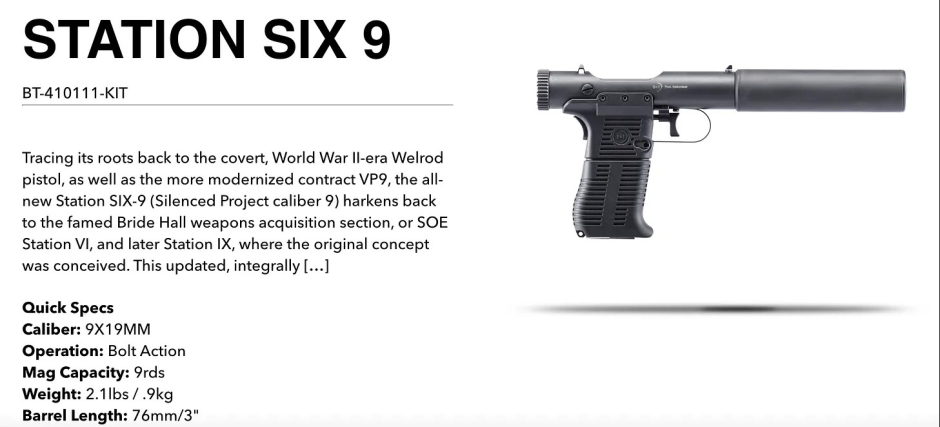
As the weapon is described on the manufacturer's website.
This updated, integrally suppressed pistol features a new grip and updated magazines, yet maintains its non-descript appearance, whisper-quiet sound signature and unique rotating bolt operation. This model in 9mm wears a 3-in. barrel. It finds its operational success as a magazine-fed, non-auto-ejecting single-shot functioning in a rotational bolt action.
The "whisper-quiet" sound made this weapon perfect for shooting someone on a Midtown Manhattan sidewalk without drawing attention. If Thompson had not approached the Hilton (he was staying at a different hotel) when another person was standing outside the entrance, drinking a coffee, it's likely that no one would have noticed the shooting for several seconds or even minutes.
The gunman apparently knew that Thompson was not staying at the Hilton but would be walking into the Hilton between 6:30 and 7:00 a.m. Note that this is fairly precise intelligence.
Why did the assassin choose the extremely risky enterprise of shooting Thompson in Midtown Manhattan instead of waiting for a lower risk opportunity near the UCH CEO's home in Minneapolis? To me, this suggests the motive to eliminate Thompson arose shortly before he attended the conference in New York.
This brings me back to my musings in my original post about this murder. If I were an NYPD homicide detective, I would consider the working hypothesis that Thompson was planning to disclose information or make an announcement at the conference that someone with power wished to remain concealed.
Yet another (wildly speculative) theory is that the assassin is somehow linked with an intelligence agency that wished to eliminate Thompson because he knows too much about U.S. federal health agency corruption. During the pandemic, Thompson was CEO of UHC's government programs, including Medicare and retiree coverage, and community and state programs providing Medicaid and other types of coverage to millions of individuals.
Medicare and Medicaid fraud assumed monstrous proportions with the passage of the CARES Act of March 25, 2020. As we noted in our book The Courage to Face COVID-19: Preventing Hospitalization and Death While Battling the Bio-Pharmaceutical Complex:
According to the U.S. Department of Health and Human Services, the CARES Act created a 20% add-on to be paid for Medicare patients with COVID-19. The Act further created a $100 billion fund that was used to financially assist hospitals, "a portion of which will be used to reimburse healthcare providers, at Medicare rates, for COVID-related treatment of the uninsured."
The CARES Act, which was hastily drafted within the context of an emergency, was reminiscent of the Emergency Economic Stabilization Act of 2008 for bailing out Wall Street, only the amount of money created ($2 trillion) for the latter crisis was a much larger sum, equivalent to 10% of U.S. GDP. As in the case of financial institutions back then, vast federal funds were created and disbursed to hospitals to assist them in dealing with the emergency. Uncle Sam paid hospitals a fee for performing a Covid test, then another fee for admitting a Covid positive patient, and then the full daily Medicare (with a 20% add-on) hospitalization rate, regardless of the patient's insurance status.
The MD and Minnesota State Senator, Dr. Scott Jensen, drew attention to this in an April 8 interview with Fox News's Laura Ingraham:
Right now, Medicare has determined that if you have a COVID-19 admission in hospital, you'll get paid $13,000 dollars. If that COVID-19 patient goes on a ventilator, you get $39,000 dollars, three times as much.
Dr. Jensen was addressing the concern that hospitals were thereby incentivized to code patients as COVID-19 admissions even if they were suffering from other illnesses or injuries. Of additional concern was the CDC's guidance:
In cases where a definite diagnosis of COVID-19 cannot be made, but it is suspected or likely (e.g., the circumstances are compelling within a reasonable degree of certainty) it is acceptable to report COVID-19 on a death certificate as "probable" or "presumed."
This created the possibility that the death of any patient-including extremely frail people with multiple co-morbidities-who also happened to present flu-like or pneumonia symptoms, could be attributed to COVID-19, even without a positive test.
In the April 8, 2020, White House press briefing, Dr. Fauci dismissed this concern as "a conspiracy theory," thereby ignoring innumerable, well-documented cases within the American healthcare system of fraud committed as a result of perverse incentives. CARES Act payments were conceived to give hospitals resources to cope with a mass medical emergency. The danger of perverse incentives lay in the fact that hospitals received a 20% add-on Medicare rate for all patients, regardless of their age, insurance status, and citizenship, even if the hospital did nothing for the patient but place him in a room with basic supportive care.
On November 2, 2020, the Centers for Medicare and Medicaid Services (CMS) announced it would pay an additional 20% add-on payment to hospitals that used new FDA-approved drugs for treating COVID-19. The first therapies that were eligible for this bonus were remdesivir and convalescent plasma (extracted from donated blood). The cost of these drugs was covered by the Medicare add-on payment. In other words, Medicare (a U.S. government funded institution) paid hospitals a 20% gratuity on the patient's entire hospital bill (already "enhanced" 20%) for using these new drugs. While convalescent plasma supplies were dependent on blood donation, remdesivir had no supply constraints and quickly became the standard hospital treatment for COVID-19. At a Medicare covered price of $3,100 per treatment course on a drug that cost about $10 per dose to manufacture, this enabled its company, Gilead Sciences, to book $1.9 billion in revenue for the fourth quarter of 2020, and $5.6 billion in 2021, making it the number one hospital drug for the year. Gilead enjoyed these sales during this period in spite of the fact that, on November 20, 2020, the WHO recommended against using remdesivir.
Over the course of 2020, it also became increasingly apparent that mechanical ventilation did not overcome the pulmonary inflammation and thrombosis causing SARS, and therefore didn't help patients. On the contrary, the vain effort to increase blood oxygen saturation with ever higher ventilation pressure often injured the patients' lungs, further contributing to their deaths. An obvious strategy for avoiding mechanical ventilation was to treat pulmonary inflammation with methylprednisolone (the established standard) and micro-thrombosis with anti-coagulants. However, neither of these therapies were recommended by the NIH in its October 9, 2020, treatment guidelines.
Could the CARES Act enhanced payments explain why hospitals insisted on sticking with the NIH's nihilistic treatment guidelines despite their low success rate? To put it more dreadfully: Could it be that hospitals refused to use the FLCCC's MATH+ (with ivermectin) protocol precisely because it could work and thereby imperil the 20% enhanced Medicare payment for COVID-19 patients, plus the 20% add-on for administering these patients remdesivir, plus the $39,000 payment for mechanical ventilation?
This originally appeared on Courageous Discourse.