By A Midwestern Doctor
The Forgotten Side of Medicine
September 16, 2025
Transgenderism has rapidly become one of the most contentious political issues in our country and due to its rapid rise, a variety of theories have been put forward to explain where it emerged from. Remarkably, I almost never see what I believe to be one of the most important facets of the topic discussed-the immense dangers of hormonal blockers routinely used in this field or the appalling history of these drugs and how again and again, they've been thrust into new markets they had no place ever being used in because of how profitable they are.
As such, when laws are periodically passed banning their use in children (which has now happened in many Red States), I rarely see the actual dangers of these drugs discussed, and when I've spoken to left-wing colleagues (including pediatricians) opposing these laws about the topic, most are genuinely unaware the drugs have negative side effects. Because of this, I believe it is vital to expose the actual truth behind these drugs.
How Hormonal Blockers Work
There are a variety of ways you can block the production of hormones in the body. Since the signal to produce sex hormones (e.g., estrogen and testosterone) begins in the brain, cutting that signal off mostly eliminates the body's production of hormones. The most powerful hormonal blockers, the GnRH agonists, work by overstimulating the brain's GnRH receptors so that they becomes "burned out" and no longer respond to the natural release of GnRH in the body, thereby short-circuiting the body's production of sex hormones (which in many cases is a permanent short circuit).
A variety of different GnRH over-activators are sold, such as Decapeptyl (Triptorelin), Lupron (Leuprorelin), Suprefact (Buserelin), Synarel (Nafarelin), Zoladex (Goserelin). Since Lupron is the most commonly used one, henceforth, I will only discuss it, but much of what I will say about Lupron also applies to the others as well.
Note: there are also numerous similar drugs which instead temporarily shut down hormone production by directly blocking the GnRH receptor (e.g., Orilissa). Additionally, there are other GnRH over-activators which are only used in animals and have similar side effects to those observed in humans.
Since testosterone fuels the growth of prostate cancer, there was a lot of research on cutting of the body's testosterone to treat it. Initially the most promising approach was to counteract testosterone with an estrogen analog ( DES) which was eventually pulled from the market because it caused a wide variety of issues (e.g., heart attacks, female cancers, and a variety of severe problems in the children of mothers who took DES-which has led many to argue the COVID-19 vaccines may become "the new DES").
Since Lupron, by burning out GnRH receptors, chemically castrates males (and thereby eliminates their testosterone), a 1984 study was conducted comparing the use of DES to Lupron for patients with prostate cancer which had metastasized to the bones and was hence likely to be fatal. It found Lupron slightly increased their survival rate (although half still were dead within two years of starting the therapy) and it had a slightly different mix of severe symptoms when compared to DES, which in turn was used to argue it was a viable alternative to DES.
When the FDA reviewed this study, the reviewers noted the study had a variety of serious issues so it was difficult to draw any firm conclusions from it. As a result ( despite the FDA knowing Lupron had real longterm risks that had not been investigated and other critical aspects of the drug like how the body metabolizes it remaining unknown to this day), Lupron was approved in 1985 as a "palliative treatment of advanced prostate cancer," a situation which is frequently so debilitating and painful for cancer patients, anything which could potentially somewhat improve it is viewed as justified.
Note: six months ago, Scott Adams, who had advanced prostate cancer, shocked the online community by saying the torture of it had made him decide upon committing suicide in a few months after an important life event had passed-providing a clear example of how dire "advanced prostate cancer" can be.
Since that time, Lupron's approval was never updated. For those interested, a detailed explanation of why that approval was overtly fraudulent and unwarranted can be found here.
Note: in addition to Lupron offering a very small survival benefit, a strong case can be made that since it is frequently observed to causes a variety of severe complications (e.g., a large increase in fatal heart attacks or diabetes), its reduction in the prostate cancer death rate is actually an artifact of it killing the patients in another manner before a slow growing prostate cancer would. This perspective for example was shared by the Vice President and Chief Scientific Officer of the American Cancer Society.
Once Lupron was approved, it use transitioned from only the most severe prostate cancers to all of them (even though, as shown by a 2009 study of 19,271 men, using Lupron actually increased the death rate). At the same time, a variety of other copycat drugs entered the market. The FDA in turn approved them (or Lupron) for advanced prostate cancer, advanced breast cancer, endometriois (along with its pretreatment prior to surgery), the pretreatment of fibroids before surgery, and preventing precocious (early) puberty.
Note: while I believe the risks of these treatments greatly exceed their benefits, it is also true that a subset of patients exist with those conditions who benefit from Lupron and suffered minimal side effects from the drug.
Additionally, a variety of other off-label uses were concocted, such as:
• "Treating" every imaginable gynecological problem (e.g., large fibroids, difficult menstrual cycles, ovarian cysts).
• In-vitro-fertilization and egg donation protocols.
Note: many young women are paid thousands of dollars to donate their eggs. Unfortunately, a portion of those donors suffer significant complications they are not warned about beforehand and then are left on their own to address. This is likely in part due to the fact Lupron is frequently part of the protocol. Likewise, significant birth defects (which Lupron has been shown to cause in the majority of pregnancies) are frequently reported following IVF-which may explain why despite Lupron being originally patented as a fertility medicine, it could never be formally approved for that use.
• Chemical castration for sex offenders (e.g., pedophiles).
• Helping children become taller (by delaying puberty so their growth plates take longer to close).
• Preventing puberty in a transgendered youth
.
Note: a more detailed list of the off-label uses can be found here. It is truly remarkable how many different tactics were used to seed these additional uses (e.g., bribing countless doctors and medical charities to promote these drugs) and likewise how many other uses (e.g., for Alzheimer's disease and Autism) came very close to becoming off-label uses as well.
In turn, there are three important things to take away from all of this.
1. While these drugs were initially developed for men (i.e., prostate cancer), they are frequently given off-label to women. This for example is why Lupron's FDA insert states its only indication is for the palliative treatment of advanced prostate cancer but it simultaneously warns against pregnant women taking it (even though it's also used for egg harvesting)
2. Despite having been on the market for decades, there is very little evidence to show these drugs actually benefit those who take them.
3. Given this, along with how incredibly toxic they are (especially to women), it raises a fairly simple question-why on earth are these drugs so popular?
Selling Lupron
Lupron's manufacturer was stuck with a rather large challenge-how could they got doctors to begin prescribing an incredibly dangerous and ineffective drug? This in turn was accomplished through one of the most overt acts of physician bribery I've seen in American medicine.
Since Lupron initially did not sell well, Lupron's manufacturer took advantage of the existing "standard" which allows chemotherapy drugs to be sold for a very high price and be "forgiven" for their extreme toxicity. This was done by reformulating Lupron into a long acting monthly shot urologists could directly administer to their (prostate cancer) patients and hence directly profit from marking up when they resold it (e.g., Medicare paid 1200 dollars per shot-or roughly 2400 in today's dollars, and in many cases urologists charged far more, all of which allowed many urologists to make hundreds of thousands of dollars per year administering the shots).
Note: TAP frequently advertised to urologists they could make over $100,000 annually selling Lupron and later cited similar figures to OBGYNs.
To further sweeten the deal, Lupron's manufacturer frequently bribed urologists and gave them free Lupron samples they "resold." This was illegal-and eventually resulted in a 875 million dollar fine...but no pharmaceutical executives going to prison.
Because Lupron was immensely profitable, more and more urologists jumped on it, and by the late 1990s Lupron treatments were costing almost a billion dollars per year and accounted for 40 percent of all Medicare payments to many urology practices in the late 1990s. To address this, in 2001, Medicare clamped down on urologists reselling discounted Lupron and in 2003 Medicare lowered the reimbursement for Lupron. In turn from 2003-2005, the rate of inappropriate use of hormonal treatment for prostate cancer dropped from 38.7% to 25.7% and many urologists at the time reported their income had been halved.
Note: one survey found 53% of the urologists who did not believe prescribing Lupron benefitted certain prostate cancer patients still prescribed the drug to them.
This Medicare crackdown on excessive Lupron prescribing for prostate cancer created a major problem for the industry. "Fortunately," since Lupron was so profitable, many others specialities appeared eager to jump on the Lupron bandwagon, particularly OBGYNs (despite the existing data on using Lupron for gynecological conditions being very poor and in many cases overtly fraudulent). This in turn led to a rapid proliferation of new off-label "uses" for the drug, such as the ones listed above. Remarkably, despite the fact Lupron has been on the market for decades, it is still extremely expensive.
Lupron hence is a very lucrative drug. However it is unclear to me exactly what the current reimbursement is for it (e.g., when I've looked online, many patients said they were billed over 10,000 dollars for a single injection).
A recent article exploring the subject found that puberty blockers can cost tens of thousand dollars per year. While insurance typically covers these drugs around 72% of the time, without insurance, according to once source, they cost $4,000-$25,000 per year and according to another source a 3 month Lupron injection is $9500 while a competing 3 month option (histrelin) is $39,000.
Similarly, a 2022 NPR article detailing a man's prostate cancer experience (where he was given unwarranted Lupron shots) reports he was charged $35,414 for the first shot and $38,398 for the second by a Chicago "non-profit" hospital, and after two years of haggling, was forced to pay the $7,000 not covered by his health insurance.
Let's compare that to how much Lupron costs ( this table designates the average wholesale price pharmacies pay for drugs):
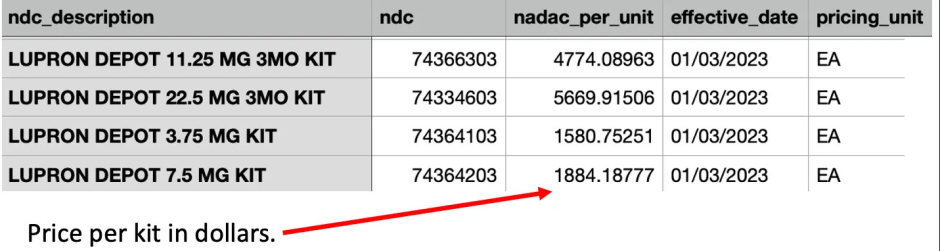
Note: these costs are unusual as they are much higher than what pharmacies typically pay for a drug (especially an older one). The above table is from 2023, and just a year later in 2024, the cost of Lupron went up almost 10%.
Since all of this demonstrates that Lupron is marked up by 5-10 times its original cost when it is resold to patients, I would argue those who provide these medications may have an ulterior motive in giving them to patients which frequently causes the drugs to be inappropriately prescribed.
Note: one of the most common stories I hear reported from Lupron victims is a tendency for doctors to gaslight them and insist their myriad of health problems could not have come from Lupron, hence making one of their greatest challenges be finding a doctor who can actually help them (or say qualify them for disability since they've lost the ability to work). I believe this is partly due to the unusual nature of their injuries and because many doctors have a direct personal investment in believing Lupron is safe and effective (as they aggressively pushed it on their patients-for instance many reported the doctor saying "are you brave enough to try Lupron?").