By A Midwestern Doctor
The Forgotten Side of Medicine
April 22, 2025
One of the most challenging things for me throughout my time in the medical field has been watching children become neurologically damaged by vaccines, and the widespread blindness of the medical profession to this issue. Unfortunately, because so much money has been spent to engineer the societal belief that vaccines do not cause autism, anyone who asserts otherwise is immediately subject to widespread ridicule, to the point it's mostly a lost cause to convince medical professionals vaccines aren't always safe. Sadly, in many cases, the only thing that can open their eyes is their own child being severely injured.
Since one of the central reasons the autism-vaccine link has always been dismissed is that there's no established mechanism to explain how vaccines could cause autism, this article will focus on that question and why there has been so much resistance to understanding what is behind the autism epidemic.
Note: this is a significantly revised and updated version of a previously published article.
Direct to Consumer Advertising
I believe much of the blindness to the toxicity of vaccines was a result of Clinton's 1997 decision to have the FTC allow direct pharmaceutical advertising to consumers. There are a lot of issues with this practice (the USA and New Zealand are essentially the only countries that allow it), and one effect it had was putting financial pressure on networks not to air stories critical of pharmaceuticals once they had become dependent on their advertising revenue.
Prior to this shift, news programs that were critical of vaccination would periodically be aired and were pivotal in awakening the public to the dangers of vaccination. Consider, for example, this 1978 program that was aired about a rushed experimental vaccine that ended up injuring a significant number of participants (and never would be aired today).
Note: while severe reactions (Guillain-Barré Syndrome) officially occurred in 1 in 100,000 people, when the vaccine came out, we saw numerous people it happened to, so I am relatively sure that figure greatly understates the actual harm.
In contrast, despite millions of people being severely injured or killed by the COVID vaccines and immense public interest in the topic, there was virtually no reporting in the mass media about the harms the vaccines were causing. Sadly, that is just one of many illustrations of how corrosive pharmaceutical advertising dollars are. For example:
•RFK Jr. was close friends with the chairman and CEO of Fox News. RFK Jr. has repeatedly shared that Ailes was very supportive of RFK Jr. producing a segment on the dangers of mercury in vaccines, but ultimately was forced to scrap the production because the majority of Fox's advertisements came from the pharmaceutical industry (e.g., 17-18 of the 22 advertisements on a typical nightly news show).
•The only Fox News host who actively spoke out against the COVID vaccines was Tucker Carlson (as he was able to leverage his position as the most popular news anchor in America to air his opinions), but was fired immediately after he aired a scathing critique of how our media had sold out the American people for Pfizer and Moderna."
Andrew Wakefield
Whenever the subject of vaccination and autism is raised (particularly within medical circles), you will immediately be told (often in a condescending manner) some variant of the following:
Andrew Wakefield was a dishonest doctor who was bribed by lawyers to torture children and publish a fraudulent and deeply flawed study that falsely linked vaccines to autism. His abhorrent actions deeply violated the profound trust we place in scientists, and tricked people into believing vaccines cause autism. Remarkably, even though his study has been totally discredited and he lost his medical license for the gross misconduct he committed, his fraudulent study cemented the lie that vaccines cause autism, and despite all the data we publish, nothing can undo the profound damage Wakefield did to science so nothing like this must ever happen again.
While most things do not get under my skin, this has become because of how nauseating it is to hear it repeatedly. This, in turn, touches on a key point. One of the most common ways the corporate propaganda apparatus ( known as the Public Relations or PR industry) persuades the public is by sculpting the narrative best suited for swaying public opinion and then blasting it on every media platform while any opposing viewpoint is forbidden from being aired. These lies then become entrenched and everyone starts to independently repeat them as though the idea were their own (e.g., we witness one of the most over-the-top PR campaigns in history to sell the COVID-19 vaccines and before long much of the populace was zealously espousing its nonsensical talking points).
Since Wakefield's study was published in 1998 (a year after pharmaceutical television advertising became permissible), it was able to initially gain immense traction in the press (as the media had not yet been bought out), but a few years later, when that monopoly had established itself, it was instead debunked on every platform.
Note: Sharyl Attkinson, a popular national news anchor for CBS and an Emmy-Award winning journalist shared that in the early 2000s, the pharmaceutical industry, feeling the pressure negative coverage of disastrous vaccination programs was creating for them, lobbied to prevent future negative coverage, and after this happened, it became impossible for her to air well produced segments which were critical of any vaccine initiative
In my eyes, there are three critical points to understand from Wakefield's experience.
First, it cemented the lie that no one had ever thought to associate vaccination with brain injuries prior to Wakefield's study (and hence that all subsequent associations were a product of Wakefield tricking them into seeing a connection that wasn't there). As the 1982 news program shows, this is clearly not true and likewise the reason Wakefield did the study was because he was approached by parents who already thought vaccines caused their child's autism.
More importantly, if you read through the early medical literature (prior to vaccine injuries becoming a taboo subject), many doctors over the decades had reported brain damage and characteristic neurological injuries (e.g., cranial nerve palsies) following vaccination that mirror what we see in vaccine-injured children now-many of which can be found within this excellent book by an eminent bacteriologist that summarized that early (forgotten) literature.
The Hazards Of Immunization (1967) by Sir Graham Wilson
2.01MB ∙ PDF file - Download
-
Second, it gave a very clear warning to every academic journal and researcher to never consider publishing anything that was critical of vaccination (as otherwise they would be raked over the coals for decades by the entire media apparatus like Wakefield was). This worked as intended (e.g., many scientists have confided to public figures that they know that autism is linked to vaccination but cannot publicly study it) and since Wakefield's study, virtually no studies have been conducted on vaccine injuries, and of those that were, none could ever be published in a"reputable"journal. Likewise, it cemented the lie the few doctored studies that get through are immediately removed (whereas for example, trial participants and clinical investigators for the HPV and COVID vaccines repeatedly provided proof fraudulent data was published but the academic journals never even issues a correction).
Note: Wakefield's study was published in one of the world's top medical journals (The Lancet). Given how controversial the subject was, it was virtually guaranteed that an exhaustive peer review was conducted of his findings and that The Lancet chose to publish the study not because"Wakefield tricked them"but rather because his data was valid and did not claim anything more than what his data clearly showed.
Third, Wakefield determined a process that appeared to be contributing to the disease process in autism and that many have since found was effective in addressing the condition. However, rather than being considered, it was blackballed and forgotten.
Do Vaccines Cause Autism?
One of the primary purposes of propaganda campaigns is to defend things that are logically indefensible, and since there are a limited number of ways to pull that off, you will gradually begin to see the ways this is accomplished. This in turn is why many were able to see through the marketing campaign used to sell the COVID vaccines, and more importantly, why so many lost their trust in the childhood vaccines they had never questioned before.
For example, if you look at the vaccine-and-autism question, a few major issues emerge:
•While many parents have observed their healthy children suddenly regress and become severely impaired immediately after a vaccine (with the regression occurring in a characteristic and replicable manner), to my knowledge, there are no reported cases of rapid autistic regressions happening immediately prior to a vaccination.
I have met a fair share of people with identical experiences to the parents in this audience.I suspect that in the near future we will see the same for those with COVID-19 injuries, and like before, almost everyone will deny they exist. pic.twitter.com/o9EtKcTgCs
- A Midwestern Doctor (@MidwesternDoc) 𝕏 x.com
In contrast, the most common argument used to dismiss a link between vaccines and autism is that"autism tends to emerge at the same age vaccines are given, so the association parents perceive is coincidental, which Andrew Wakefield tricked them into seeing."If this were indeed true, there would be a roughly even distribution of autism cases before and after vaccination rather than what we actually observe.
2. Over the past 50 years, there has been an exponential increase in the rates of autism (e.g., HHS Sec. RFK Jr. announces findings of autism survey conducted by CDC: LIVE ). This rapid increase suggests something is causing it, and more importantly, that it is absolutely urgent for us to figure out what that something is as each autism case is immensely costly to society. This is not sustainable once it starts to affect a significant number of children. However, rather than identify that cause, the scientific community, for decades, has simply said"we need more research"to figure out what it is (while simultaneously declaring it is definitely not vaccines despite vaccines being by far the most probable culprit)."
Note: while I believe the strongest case can be made for vaccines causing the autism epidemic, there are a few other factors (e.g., excessive prenatal ultrasounds) that data suggest may also play a contributing role."
3. The most common explanation given for the explosion in autism is that"it's genetic,"and as the years go by and billions are spent on autism research, more and more genes are identified that are associated with autism. This train of thought, however, ignores:
•Despite all that research, the"autism gene"has never been found.
•If autism suddenly became over 100 times more common in 1-2 generations, it is impossible that this could have been due to a genetic shift.
•In addition to this rapid change arguing for an environmental toxin (rather than genetics) causing the autism epidemic, many of the genes"linked to autism" share the common thread of increasing one's sensitivity to environmental toxins.
Note: Peter Hotez is often used as a media attack dog to discredit anyone linking vaccines to autism and frequently cites his book" Vaccines Did Not Cause Rachel's Autism"as an authoritative debunking of any links between the two. I read Hotez's book and noticed that he never proved his claim (rather, he just said it didn't make sense to him how autism could be anything except genetic) and described a classic sign of vaccine encephalitis (a continual, very loud, and piercing cry) prior to his daughter's autistic regression.
4. While many studies are published debunking the link between vaccines and autism, they never directly assess the question. Independent studies (whose validity is always questioned) continually find an indisputable link between the two ( along with vaccination being linked to many other chronic illnesses). A schism like this would argue for a robust trial to settle the question (e.g., a randomized one that compared a group of vaccinated and unvaccinated children from birth), but each time that is proposed, it's shot down because"it's not ethical to withhold lifesaving vaccines from children"when the next best alternative is proposed (access to the CDC's database that compared vaccinated children to unvaccinated children), for some reason, that too is always shot down.
Note: in one instance, a CDC whistleblower came forward and showed that after the CDC conducted a study to disprove the link between autism and vaccines, when they discovered it actually caused autism, the study was doctored to conceal this.
All of this hence suggests vaccines are strongly linked to autism and helps to explain why both the media and much of the Democratic leadership went hysterical after RFK Jr. stated he planned to conduct robust studies to determine what was actually causing the autism epidemic.
Note: For those interested in learning more about how vaccines cause autism, I would strongly recommend reading Steve Kirsch's article. He does a good job of concisely presenting some of the most compelling evidence (e.g., specific cases where vaccination was irrefutably linked to autism and the hundreds of papers on the subject).
The Toxicity Bell Curve
Whenever living organisms are exposed to a toxin (at least at levels below a certain lethal dose), the responses to the toxin, will greatly vary, with some having no reaction, some having minor reactions, some having moderate reactions, and some having severe reactions. In most cases, the subtle reactions are much more common than the severe reactions, leading to a distribution like this:
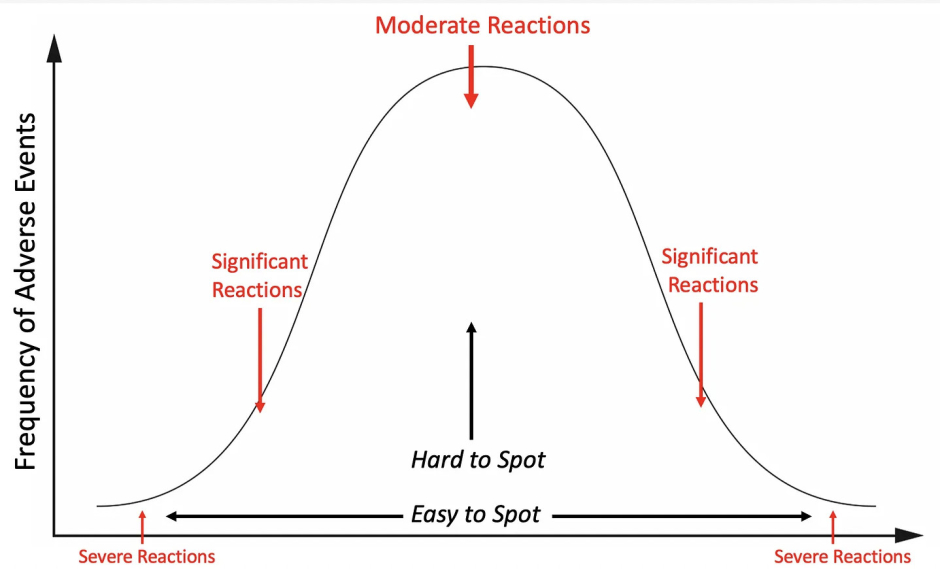
This, for example, was why I knew a lot of people would develop complications from the COVID-19 vaccines. I received a few phone calls from friends around the country of a relative who'd"died suddenly"after the vaccines (which, much later, was confirmed by polling that showed 34% of those vaccinated reported minor side effects and 7% reported major side effects).
In the case of vaccine brain injuries, a similar pattern emerges, where typically the neurological changes are subtle (and often only noticeable by comparing vaccinated children to unvaccinated children), while in a small number of cases they are quite severe. Likewise, with autism, some children have total developmental disability requiring permanent full-time care from their parents, while others simply have non-verbal deficiencies and awkward social impairments but are generally functional (e.g., Asperger's syndrome like that seen in Elon Musk). Because of this, autism is described as"being on a spectrum"(and hence called "Autism Spectrum Disorder").
Since the public relations field is always looking for ways to sell illogical and unsellable ideas to the public, a limited number of tactics exist to facilitate this. One common approach is to enshrine an ambiguous term within the public consciousness and then, depending on the context, use different meanings of the word so that those promoting the idea can effectively have their "cake and eat it"as one definition is used when it benefits them, and another is used when it's necessary to get out of responsibility for their misdeeds
Through labeling autism as a spectrum, that ambiguity has been deliberately enacted for autism, as on one hand, people know to refer to the severely developmentally delayed children (who comprise roughly 25% of those with"autism") as being autistic, but at the same time the other definition can be pivoted to so that:
•Anytime the massive increase in autism is mentioned, it can be dismissed and attributed to far more children with less severe forms of autism being diagnosed.
•Anytime the devastating consequences of autism are highlighted, they can be dismissed by focusing on cases of individuals with high-functioning autism.
For example, shortly after Secretary Kennedy 𝕏 announced a massive initiative to study the causes of autism, and mentioned the profound disability many children with autism experience, Elizabeth Warren (who has consistently been promoting vaccine-industry talking points ever since RFK Jr. was nominated) 𝕏 shared this:
Fortunately, most of the public saw through this and most of 𝕏 the comments were people telling Warren she was an awful person and posting videos of their children with severe autism.
Note: all of this illustrates why it is so problematic (and likely intentional) that we do not have a clear definition of what constitutes autism. Likewise, it also touches upon a common tactic by industry to normalize the harms their products cause so they can never be questioned and in time not recognized either.
Vaccine Autism Research
Note: This section was sourced from a compilation of 224 studies that can be viewed here, the book Miller's Critical Review of Vaccines Studies and Chapter 5 of How To End The Autism Epidemic. Of these, I believe the final book provides the most concise (but detailed)‚ summary of those mechanisms.
Much of the research on the link between vaccines and autism has focused on the following areas:
1. Immune-activating events are repeatedly correlated with an increased likelihood of developing neurological developmental disorders like autism."
2. Increased blood levels of inflammatory cytokines (e.g., "Plasma levels of IL-1β, IL-6, and IL-8 were increased in children with ASD and correlated with regressive autism, as well as impaired communication and aberrant behavior"). Autistic individuals also appear to have a predisposition to developing inflammatory immune responses
3. Vaccinations create inflammation in the brain, and inflammation in the brain is linked to autism. This neurological inflammation is often chronically active in the brains of autistic individuals and appears to be most specifically linked to aluminum and the measles virus component of the measles, mumps, and rubella (MMR) vaccine. For example, the vaccine measles virus was observed to correlate with the production of autoantibodies to brain tissue, increased levels of measles antibodies were found to be significantly higher in autistic children (but not antibodies to mumps or rubella), and live measles viruses were found in immune cells of autistic children with inflammatory bowel disorders. The strongest case for the link between the measles vaccine virus and autism came from the discovery that vaccines with the measles component have triggered severe brain injury and death but those with only the mumps or rubella components have not."
4.Enlarged brains are also often associated with autism (likely due to that inflammation). This swelling may play a key role in the pathology of autism and explain why certain individuals are more susceptible to it.
5. The brain inflammation induced by vaccines occurs at a critical period of brain development.
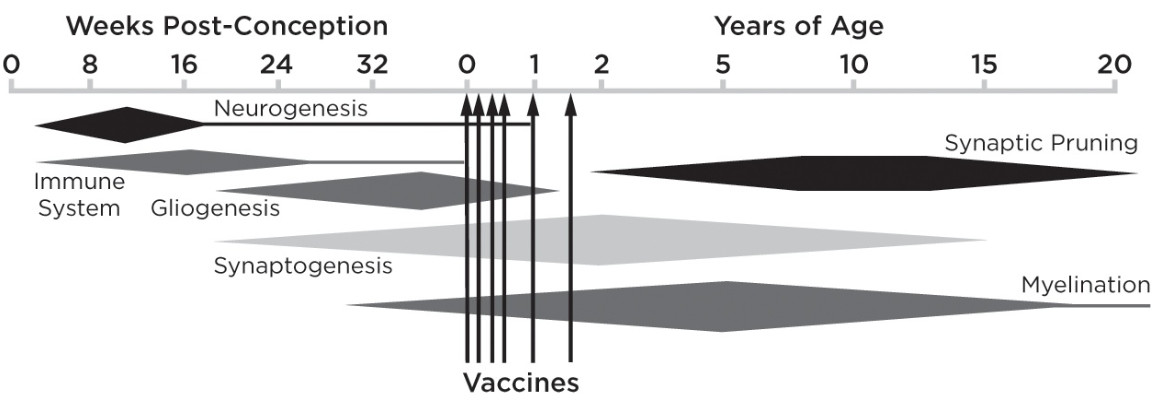
This argues for providing the vaccines later in a more spaced-out fashion; something that many have observed dramatically lowers the rate of adverse neurological reactions to vaccines. Unfortunately, safer vaccination practices are never even discussed as doing so would be a tacit admission that vaccines are not 100% safe. This is likewise why I believe defenders of the orthodoxy (e.g., Peter Hotez) devote so much energy toward attacking the parents desperately trying to treat vaccine injuries in their autistic children.
6. Pathologic alterations in the gut microbiome (that increase the likelihood of autoimmunity), a dysregulated immune response (that includes responses in the gastrointestinal tract and responses toward a variety of common allergens such as those within foods), along with a variety of gastrointestinal symptoms are observed in autistic individuals.
7. The neurotoxicity of mercury, the tendency of autistic individuals to have elevated mercury exposures, and autistic individuals have difficulty detoxifying mercury. All of the previous has also been found for lead, another toxic heavy metal..
8. Aluminum, an inflammatory and neurotoxic vaccine adjuvant, when injected into mice, was found to rapidly trigger symptoms similar to those observed in neurological developmental disorders. Aluminum was also found to trigger a fourfold increase in brain levels of IL-6, the inflammatory cytokine most closely linked to autism.
9. Aluminum is found in elevated levels in the brains of autistic individuals. For example
"The aluminium [it is spelled this way in England] content of brain tissue in autism was consistently high. The mean (standard deviation) aluminium content across all 5 individuals for each lobe were 3.82(5.42), 2.30(2.00), 2.79(4.05) and 3.82(5.17) μg/g dry wt. for the occipital, frontal, temporal and parietal lobes respectively. These are some of the highest values for aluminium in human brain tissue yet recorded and one has to question why, for example, the aluminium content of the occipital lobe of a 15 year old boy would be 8.74 (11.59) μg/g dry wt.?"
10. Impairment of the blood-brain barrier is observed in autism (increased permeability of the gut barrier has also been observed).
11. A dose-response relationship exists between specific vaccinations and the likelihood of autism. For example:
The average MMR coverage for the three countries fell below 90% after Dr. Wakefield's infamous 1998 publication but started to recover slowly after 2001 until reaching over 90% coverage again by 2004. During the same time period, the average autism spectrum disorder prevalence in the United Kingdom, Norway and Sweden dropped substantially after birth year 1998 and gradually increased again after birth year 2000.
12. Likewise, a dose-response relationship exists, finding autism is more likely to occur in premature infants (who effectively receive a higher dose since they are smaller) and those who receive multiple vaccinations simultaneously. For example:
No association was found between preterm birth and NDD [neurological developmental disorders] in the absence of vaccination, but vaccination was significantly associated with NDD in children born at term (OR 2.7, 95% CI: 1.2, 6.0). However, vaccination coupled with preterm birth was associated with increasing odds of NDD, ranging from 5.4 (95% CI: 2.5, 11.9) compared to vaccinated but non-preterm children, to 14.5 (95% CI: 5.4, 38.7) compared to children who were neither preterm nor vaccinated.
Note: This is also the same pattern that has been observed with vaccines causing sudden infant death syndrome (SIDS).
13. A variety of genetic and metabolic abnormalities have been extensively studied in autism. Many of these (e.g., those relating to glutathione) correlate with impaired detoxification and mitochondrial dysfunction, conditions both frequently observed in autistic individuals.
One important thing to understand about these points is the difficulty of identifying a single precise cause of autism without a broader picture of what causes it. For example, many were convinced that mercury in vaccines was the primary cause of autism, and there was quite a bit of research that substantiated this link. Yet, despite vaccine mercury being mostly pulled from the market, autism has increased rather than decreased since thimerosal (mercury) was pulled.
Wakefield's Paper
While Andrew Wakefield's infamous Lancet paper is widely referred to in the media, I find very few of those who disparage it actually ever read it. To quote it:
Methods: 12 children (mean age 6 years [range 3-10], 11 boys) were referred to a paediatric gastroenterology unit with a history of normal development followed by loss of acquired skills, including language, together with diarrhoea and abdominal pain. Children underwent gastroenterological, neurological, and developmental assessment and review of developmental records. Ileocolonoscopy and biopsy sampling, magnetic-resonance imaging (MRI), electroencephalography (EEG), and lumbar puncture were done under sedation. Barium follow-through radiography was done where possible. Biochemical, haematological, and immunological profiles were examined.Findings: Onset of behavioural symptoms was associated, by the parents, with measles, mumps, and rubella vaccination in eight of the 12 children, with measles infection in one child, and otitis media in another. All 12 children had intestinal abnormalities, ranging from lymphoid nodular hyperplasia to aphthoid ulceration. Histology showed patchy chronic inflammation in the colon in 11 children and reactive ileal lymphoid hyperplasia in seven, but no granulomas. Behavioural disorders included autism (nine), disintegrative psychosis (one), and possible postviral or vaccinal encephalitis (two). There were no focal neurological abnormalities and MRI and EEG tests were normal. Abnormal laboratory results were significantly raised urinary methylmalonic acid compared with agematched controls (p=0·003), low haemoglobin in four children, and a low serum IgA in four children.
Interpretation: We identified associated gastrointestinal disease and developmental regression in a group of previously normal children, which was generally associated in time with possible environmental triggers.
Asperger first recorded the link between coeliac disease and behavioural psychoses. 4 Walker-Smith and colleagues 5 detected low concentrations of alpha-1 antitrypsin in children with typical autism, and D'Eufemia and colleagues 6 identified abnormal intestinal permeability, a feature of small intestinal enteropathy, in 43% of a group of autistic children with no gastrointestinal symptoms, but not in matched controls. These studies, together with our own, including evidence of anaemia and IgA deficiency in some children, would support the hypothesis that the consequences of an inflamed or dysfunctional intestine may play a part in behavioural changes in some children.
Intestinal and behavioural pathologies may have occurred together by chance, reflecting a selection bias in a self-referred group; however, the uniformity of the intestinal pathological changes and the fact that previous studies have found intestinal dysfunction in children with autistic-spectrum disorders, suggests that the connection is real and reflects a unique disease process.
We did not prove an association between measles, mumps, and rubella vaccine and the syndrome described...Further investigations are needed to examine this syndrome and its possible relation to this vaccine.
In short, Wakefield (who at the time was a highly respected gastroenterologist) discovered that:
•Unusual bowel inflammation was frequently observed in children who'd had a rapid autistic regression following vaccination.
•Existing evidence showed gastrointestinal issues could cause neuropsychiatric changes.
•The data in his study suggested this topic should be investigated further.
Following Wakefield's study, another team (with Wakefield's help) conducted a 2002 study that found developmentally delayed children had bowel inflammation that appeared to be linked to the measles virus present in the bowel, in turn suggesting the MMR vaccine (specifically its attenuated measles virus) was directly causing that bowel inflammation. Like Wakefield's original paper, this study has been heavily criticized by the scientific community."
In my eyes, this research being swept under the rug has been immensely unfortunate as:
•It provides a potential mechanism to explain the pervasive inflammation seen in vaccinated children.
•It helps to explain why parents often find one of the most helpful things they can do is remove food allergens (as inflamed and permeable bowels are much more sensitive to them).
However, since all of this was buried, most parents never learned about the simple dietary things they could do to improve their child's autism.
Note: the MMR vaccine (likely due to its live measles component) has been the vaccine most strongly correlated with autistic regressions. However, many other vaccines have also been associated with devastating brain damage.
How Do Vaccines Cause Autism?
In my eyes, there are three core reasons why vaccines cause autism:
- They create chronic neurological (or possibly gastrointestinal) inflammation.
- They cause a zeta potential collapse.
- They create a sustained cell danger response in the body.
- Additionally, each of these can cause the other two, making their separation somewhat arbitrary.
There are a few important correlates of these three processes.
The first is that things besides vaccines can also trigger each of these to occur (e.g., congenital rubella infections can also cause developmental delay). The difference with vaccinations is that they are highly likely to cause each of them and more importantly, are something (almost) every child is exposed to. As a result, the most common trigger for autism is vaccination, but other things can also serve as the trigger for each of these processes. This helps to explain much of the confusion about exactly what causes autism.
Secondly, these are the same critical processes that underlie many other diseases such as Alzheimer's and the myriad COVID-19 vaccine injuries. One of the most compelling data points I have come across supporting this relationship comes from Ed Dowd's recent discovery of England's disability claims data, within which the rate of adult autism requiring disability support spiked in parallel with the vaccine rollout.
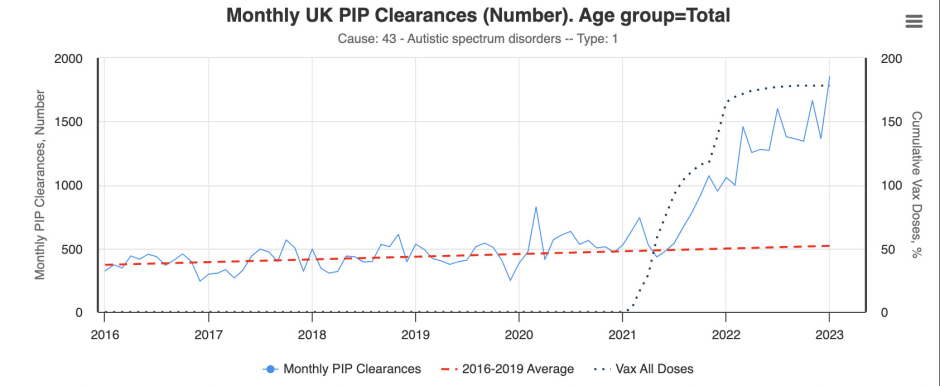
Note: This dataset is for claims in individuals aged 16 and older.
Third, most of the treatments I have seen that effectively treat autism ultimately address one or more of these three processes. For example, one large survey of parents with autistic children found virtually all the medications they were prescribed did not help, but four things did:
•Addressing food allergies (e.g., by removing gluten from the diet).
•Addressing an underlying Candida infection.
•Addressing genetically impaired methylation.
•Removing heavy metals from the body.
There are a few other treatments I have also seen significantly improve regressive autism, and I believe each of those treatments likewise improves one or more of the three critical processes. Many of those treatments have also been quite helpful in treating COVID-19 vaccine injuries, so I believe they are even more important to understand now.
Inflammation
One of the most common side effects of vaccinations is autoimmune disorders. This makes sense since vaccines work by stimulating the immune system to respond to something, and autoimmune disorders result from excessive activation of the immune system. Although there are many different mechanisms at work here, at this point, I believe the primary ones are as follows:
1. If the immune system develops an immune response to a target protein (an antigen), it will often also develop an immune response to other antigens with similarities to the target antigen, a process known as molecular mimicry that is well recognized to occur with certain infectious organisms (e.g., the bacteria that cause rheumatic fever). Certain vaccine antigens have a higher overlap with human tissue and hence have a higher rate of autoimmune complications.
Note: One of the major concerns with the COVID-19 vaccines was that its spike protein antigen had an extremely high degree of overlap with human tissue. Although this concern was repeatedly raised (e.g., consider an early 2021 paper), it was ignored, much to the detriment of the many COVID-19 vaccine recipients who developed autoimmune complications from the vaccine.
2. Vaccines are typically composed of a target antigen under the theory that exposing the body to the antigen will eventually cause it to develop an immune response to an infection that also has that antigen. Antigens tend to be expensive to produce, so it is often not economically viable to produce enough of the antigen for each vaccine to elicit the needed antibody response.
There are two common solutions to this approach. The first is to create a self-replicating antigen (e.g., with an infectious virus that contains the antigen or an mRNA gene therapy) so enough of the antigen is produced to elicit an immune response. The second approach is to use an adjuvant—a cheap compound like aluminum that provokes the immune system to attack anything there, thereby significantly decreasing the amount of antigen needed and thus the cost of the vaccine.
The problem with adjuvants is that they will also often provoke the immune system to develop undesirable responses as well (e.g., allergies to pollens circulating at the time of vaccination or autoimmunity to human tissue resembling parts of the vaccine antigen).
3. In medicine, it is often expensive and time-consuming to prove a medication will yield a long-term benefit. For this reason, "surrogate markers," changes that appear quickly and are assumed to correlate with improved health benefits, are evaluated instead. Unfortunately, in many cases, changes in surrogate markers do not actually correlate with a tangible benefit.
In the case of vaccines, the surrogate marker is antibody formation. This creates a situation where vaccine manufacturers do whatever is needed to create an antibody response—something that can often be highly problematic. For example, with the HPV vaccine, a major design problem was that it did not elicit a sufficient antibody response. This problem was "solved" by using a stronger aluminum adjuvant that achieved the desired surrogate marker but also had the side effect of creating an extremely high rate of autoimmune complications in the HPV vaccine recipients (making it arguably the most dangerous vaccine on the market prior to the COVID-19 vaccines).
Note: I wrote a detailed article on the link between vaccines and autoimmunity here, while an even more detailed explanation can be found within this textbook.
The Cell Danger Response
Previously, I wrote a series that:
• First described the cell danger response (CDR).
• Then explained the existing approaches for treating a persistent CDR localized to a specific tissue (something that is often necessary to heal otherwise chronic musculoskeletal injuries).
•Then concluded with methods for treating a systemic sustained CDR (e.g., methods used to treat spike protein vaccine injuries).
Since a persistent CDR is often the underlying cause of a variety of chronic illnesses and functional impairments that significantly affect individuals' quality of life, the CDR both provides a helpful context to understand why so many different things can cause the same illness and why the same trigger can cause so many different illnesses, many of which persist years after the initial trigger has disappeared. What follows is an abridged summary of those three articles.
When cells are threatened by something in their environment, they will often switch to a defensive mode where the cells attempt to protect themselves rather than performing their normal functions. This process is orchestrated by the mitochondria, which switch from providing the energy to power the cell into an inflammatory form that produces the metabolites necessary to defend the cell from microbial invaders.
When the CDR is triggered, it should go through an inflammatory phase (CDR1), which is followed by a proliferative and regenerative phase (CDR2), and then an integrative phase where the cell gradually resumes its normal function (CDR3) and then exits the CDR. This cycle is essential for the survival of the human body, and many therapies work by inducing it to repair tissue. However, in many cases, when the CDR is triggered, instead of it completing, cells get trapped in either CDR1, CDR2, or CDR3, leading to chronic illnesses characteristic of the specific frozen and unresolved CDR phase.
The CDR model is extremely useful in clinical practice for a few reasons:
•First, it helps to explain many of the mysteries in treating complex chronic illnesses. A classic example would be that integrative physicians typically assume the mitochondrial dysfunction they see associated with a chronic illness is the cause of the illness and hence attempt to treat it by providing mitochondrial supports, an approach that often either does not work or worsens the patient's condition.
Note: Each of the common genes known to strongly increase the risk of autism can be shown to play a role in CDR signaling or maintenance. This helps to explain why so many different genes have been found to be connected to autism and why they did not typically cause autism until the trigger of mass vaccination was also present. Likewise, the wide range of metabolic abnormalities seen in autism overlap with the metabolic changes created by the CDR.
•Second, a sustained CDR is often the primary cause of autoimmune disorders. Conversely, factors known to trigger autoimmunity (e.g., an immune-stimulating event) often are also "dangers" to cells that trigger the CDR.
•Third, many degenerative conditions (e.g., Alzheimer's or a non-healing tendon) result from cells being trapped in a dormant state where they shut down and thereby neither heal nor resume their normal function. As a result, regenerative medicine's trick for treating many different chronic conditions characterized by a dramatically reduced functionality of the body is to "wake cells up out of the CDR."
•Finally, the CDR helps guide how to treat chronic illnesses and how to recognize which things are important to address and which should be left alone because they are simply the result of the body's compensation for an underlying issue.
Note: I primarily reference the work of Dr. Robert Naviaux. Others have also researched the process Naviaux termed the CDR and given it different names.
Autism, for instance, is characterized by cells trapped in the CDR, and many of the most successful approaches I've seen used for treating autism all treat the CDR. Naviaux in turn conducted multiple studies demonstrating that one pharmaceutical drug blocked the CDR, and when used in autistic animals and then human beings, significantly improved the condition while the drug remained active—a result that to my knowledge has never been found in clinical trials of any other therapy for autism. Sadly, despite years of research on this subject, the drug is impossible to obtain in America.
Note: Excluding Naviaux's approach, every method I have seen that I believe effectively improved autism was never feasible to test in a formal clinical trial.
My renewed interest in the CDR arose after I saw rapid improvements in long COVID and vaccine-injured patients (e.g., someone who had been on oxygen for months no longer needing oxygen within minutes) from one of the treatments we previously had success treating severe COVID-19 cases with. I spent a while trying to figure out why that improvement could be occurring, and eventually concluded it had to be because an unresolved CDR was being rapidly resolved.
Since the CDR is known to be triggered by toxic dangers to cells (e.g., the spike protein), especially after repeated cellular exposures to a danger (e.g., from synthetic mRNA that persists in the body and continually produces new dangerous spike proteins), this seemed plausible. After I contacted a few leading experts in this area, they all told me their vaccine-injured patients were characterized by a sustained CDR that could not resolve on its own. I then asked around more and found out that the same approach we were using to treat the CDR in spike protein illnesses was also treating a variety of complex (and otherwise impossible to treat) autoimmune disorders. It also took a bit longer, but I was eventually able to also find clinicians who were using it to treat autistic children and each reported remarkable improvements from it (much of which they had video footage to corroborate).
For all of these reasons, I believe a sustained CDR triggered by the danger vaccines present to the body is a core component of autism (immune-activating events trigger the CDR). However, while addressing the CDR can often significantly improve conditions it causes, the benefit is often temporary unless the underlying cause is addressed so the cells no longer have a need to reenter the CDR.
Zeta Potential
Most fluids in nature are colloids (particles suspended in water). With a colloid, two factors are always at play: forces that clump the colloid's particles together and forces that separate (disperse) them. In most cases, the primary determinant of a colloid's dispersion—quantified through zeta potential—is whether the negative charge surrounding each particle is sufficient to prevent those particles from clumping together.
Since the fluids within the body are colloidal systems, once the zeta potential is no longer sufficient to prevent clumping (agglomeration), the fluids to varying extents solidify and create a variety of problems for the body. This is the easiest to understand with blood, as when the zeta potential declines, blood cells will separate from the plasma, clump together, and stop flowing with the circulation.
At this point, I believe the physiologic zeta potential is one of the primary determinants of health. This is because many different diseases (particularly those that cause one to get hospitalized) result from impaired zeta potential, and that many of the consequences of aging come from a gradual impairment of the kidney's ability to maintain the physiologic zeta potential. In my own practice, I've found treating zeta potential is often one of the most useful things I can do for patients who show up, so the applications of this concept are very broad.
When I started studying COVID-19, I realized that the disease had all the clinical signs of being extremely disruptive to the physiologic zeta potential of the body (which I believe was why COVID-19 was often so dangerous). After more research, I concluded that this was likely due to the strong positive charge on the spike protein, and since then have found papers corroborating this theory and that restoring zeta potential is often critical for treating both COVID-19 and COVID-19-vaccine injuries.
The individual who first linked vaccine injuries to poor zeta potential was Andrew Moulden. Moulden was a Canadian Neurologist (and psychiatrist) who also had an extensive research background (e.g., a Master's and PhD) in the neurocognitive development of children and adolescents, behavioral disorders, neurobehavioral assessment of brain, and detecting acquired brain injuries.
Moulden observed that children who were vaccinated would frequently present with neurological signs of having had a stroke following vaccination; unfortunately, while those signs would often be recognized in adults, they were typically ignored in children. Likewise, I have seen many of the same injuries Moulden described in children (especially abducens nerve palsies) develop in friends of mine who received the COVID-19 vaccine.
To try and explain these observations, Moulden drew on decades of previous research into blood clumping and the various diseases it caused (discussed here). He concluded that vaccines diminished the zeta potential of the recipient, causing their blood to clump together and obstruct the circulation of regions of the brain with the weakest blood supplies, thereby triggering microstrokes that were too small to detect with conventional imaging techniques. Additionally, he found evidence suggesting the microstroke issue was worsened by immune activations because white blood cells (which are larger than red blood cells) would migrate into the small blood vessels and obstruct their flow, something he termed MASS.
Moulden then mapped out the most common microstrokes that would occur (due to the nature of their blood supply). In this, he noticed that many children who developed severe neurological disorders like autism simultaneously showed clinical signs of having had microstrokes, leading him to conclude those microstrokes were causing a variety of brain injuries, including autism and SIDS.
Note: Much like the gaslighting around autism, over a century of robust evidence (discussed) has emerged showing vaccines cause the "inexplicable" sudden infant death syndrome—but nonetheless has been buried. A strong case can be made that vaccine-induced microstrokes disrupt the respiratory centers of the brain, which leads to the infant suffocating unless a hospital happens to be monitoring the infant and can initiate respiratory resuscitation. Remarkably, despite numerous studies showing this respiratory suppression occurs following vaccination, there is virtually no awareness of it in the medical field.
Since working to bring attention to this issue, many readers have also contacted me to share their own experiences of this.
Hello, absolutely love your work. I saw that you referenced some of Dr Andrew Mouldon's work in one of your articles. My now 25 year old son is autistic with severe learning difficulties. He is non verbal and has the mental age of about 2. After his 3 month jabs - like straight after - within a day or two, his left eye turned inwards. Doctors ofcourse told me this was unrelated and "just happens". It took me 20 years to find Dr Mouldon's work and realise that this is a common side effect. Strabismus. I now see misaligned eyes in youngsters all the time. I feel that if this were more widely known, it may alert more parents to vaccine damage, since it's a very obvious physical manifestation of vaccine injury.
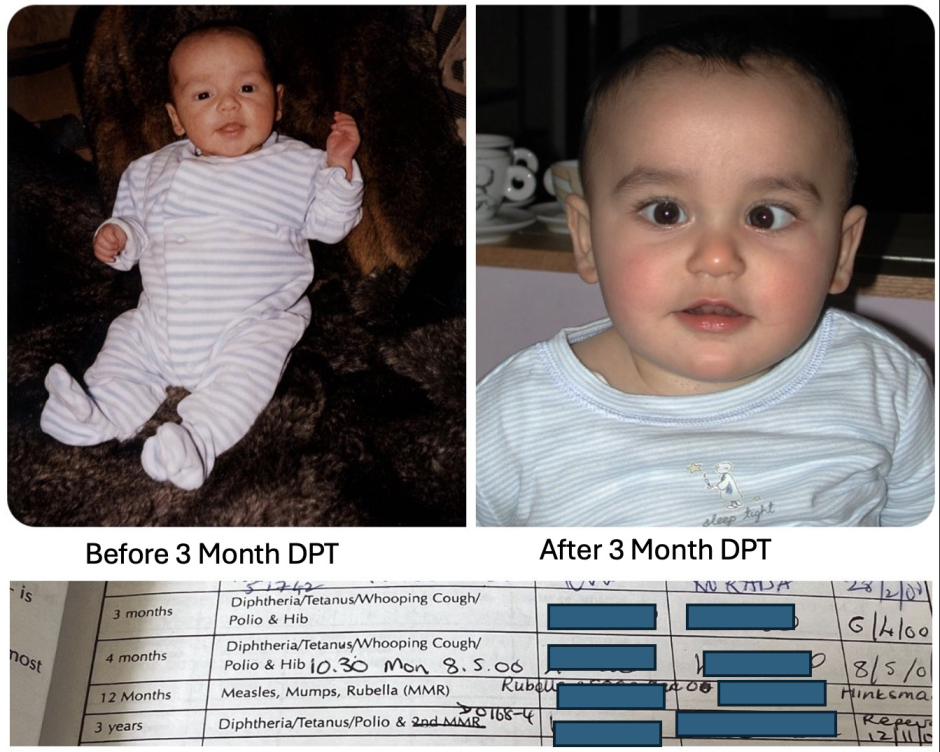
When I posted about my son from my now deleted Twitter account, a lady responded with these pictures before and after. The change came after her 4 month vaccines. Her daughter has severe learning difficulties.

Note: One of the most frustrating things about this topic is that prior to it becoming taboo to question vaccine safety, as Sir Graham Wilson's review of the older medical literature shows, many doctors noticed these cranial nerve abnormalities and brain injuries following vaccination (which at the time they attributed to inflammation and edema around the nerves compressing them). Now, however, most doctors can't see these changes. Likewise, a strong case can be made that many of the characteristic behaviors autistic children display are a natural consequence of either a cranial nerve dysfunction (discussed further) or painful brain swelling and inflammation that causes it to push against the skull (that when addressed frequently improves autism)—but within the medical field, there is virtually no awareness of this.
One of the most important things about Moulden's model was that like the CDR, it was a universal mechanism of harm and things besides vaccines (e.g., a congenital rubella infection) could also cause those dangerous microstrokes to happen. Additionally, certain vaccines ( Gardasil, Anthrax and I would argue the original Smallpox vaccine) had a much greater propensity to cause the same microstrokes that the COVID-19 vaccines have now made us all aware of, and likewise tended to most frequently cause neurological injuries.
Conversely, those who already had an impaired zeta potential were the ones most likely to have severe reactions to vaccines because they could not tolerate additional impairment of their physiologic zeta potential. This, for example, characterized the patients I have seen who were admitted to the hospital for a complication caused by a traditional vaccine and why the elderly (who have a baseline impairment of their zeta potential) are so much more vulnerable to conditions like the flu that consistently worsens the physiologic zeta potential, hence bringing vulnerable individuals past the agglomeration threshold that they can tolerate.
Note: After discovering this mechanism of injury, Moulden switched his focus to trying to treat it, but shortly before he had planned to release his treatment, died unexpectedly and many have since tried to figure out what he had discovered. Based on studying his work and talking to friends who knew him shortly before his death, I believe Moulden's approach was based around restoring the zeta potential of vaccine-injured children, something that is much easier to do with the tools available now than those that were known when Moulden was still alive.
Interrelated Pathologies
My colleagues who actively work with the CDR in practice believe it goes hand in hand with zeta potential and that the CDR often cannot be treated unless the fluid stagnation inside a patient is addressed (e.g., Lyme and mycotoxins both frequently cause stagnation because their positive charges impair zeta potential). Furthermore, in many cases, the loss of blood flow to, or drainage from tissues can be sufficient to trigger the CDR. In general, we believe one of the biggest treatment oversights made by integrative doctors who work with complex illnesses is the doctors' failure to address the lymphatic stagnation that results from a zeta potential collapse in their patients.
Note: While treating the CDR will improve many symptoms of a disease, especially if the trigger of the CDR (e.g., a chronic infection) is still present and treated as well, treating it will not address existing damage, such as that previously caused by microstrokes. This is why the animal studies Naviaux conducted found his drug improved many symptoms of autism but did not improve those resulting from damaged and lost brain tissue. Likewise, my colleagues have found many of the core symptoms of autism can be improved with approaches directed at the CDR or zeta potential that reactivate dormant brain cells, but it is much more challenging to treat specific neurological deficits resulting from previous microstrokes.
I also believe impaired zeta potential goes hand in hand with autoimmunity. This is because:
•The existing diagnostic system that best encapsulates impaired zeta potential is "blood stasis" from Traditional Chinese Medicine. TCM links blood stasis to a variety of autoimmune conditions.
•Lymphatic stagnation will cause autoimmunity. I believe a key reason why blood stasis is linked to autoimmunity is because lymphatic stasis will exist in parallel to blood stasis as both result from the same impaired physiologic zeta potential.
•Inflammatory states (as shown by the ESR test) reduce the zeta potential of the blood.
•Inflammatory activation triggers MASS that creates microstrokes, especially in the setting of poor zeta potential.
•Aluminum, the most commonly used vaccine adjuvant, is also the element with the greatest adverse effect on zeta potential (aluminum's coagulating ability is orders of magnitude greater than any other element).
•I suspect aluminum's ability to disrupt zeta potential is why it functions as such an effective adjuvant. This is because many infectious organisms also create a localized disruption of zeta potential and hence any disruption of zeta potential serves as a universal signal to activate the immune system.
Note: One of the reasons why aluminum is so problematic is because macrophages will treat it as an invading microbe and eat it. However, since they cannot digest it, the macrophages will keep the aluminum inside them and eventually deposit it in specific parts of the body (e.g., where the macrophage eventually dies). For reasons that are not fully understood, the macrophages predominantly concentrate aluminum in critical tissues in the body (e.g., the brain and spleen) and are more likely to do this when smaller doses of aluminum are used, thereby allowing a small dose of aluminum to become a toxic dose. As such, a major problem with both aluminum and the mRNA gene therapies is that they do not obey the classic assumptions in toxicology (e.g., that toxicity increases directly in proportion to the initial dose).
Presently, I believe the reason why both zeta potential and the CDR are such frequent causes of chronic illness is because each evolved in an era when we had far fewer stressors on our system. In the case of the CDR, while protective, if it is repeatedly triggered, it becomes more likely for cells to become stuck in the CDR. While an increasing sensitivity to environmental dangers was helpful in the past, since we are now exposed to too many triggers for the CDR, many are now to varying degrees trapped in the CDR.
In the case of zeta potential, the body ideally wants to have a zeta potential slightly above the threshold that will cause blood clumping and then clotting to occur, as this saves you from otherwise fatal bleeds. However, because we are now exposed to so many zeta-potential-disrupting toxins, the negative charge our bodies evolved to contain is often no longer sufficient to keep us above the critical agglomeration threshold.
Furthermore, I believe the three mechanisms outlined here, inflammation, an unresolved CDR, and impaired zeta potential, are also the primary causes of aging. To this point, one of the most common side effects of a COVID-19 vaccine injury is that individuals report that it seemed as though their bodies had aged significantly, something also observed by pathologists who had performed autopsies on individuals killed by the COVID-19 vaccines.
Conclusion
Many have argued an epidemic of neurological and autoimmune disorders characterize the modern age. For example:
Under Dr. Fauci's leadership, the allergic, autoimmune, and chronic illnesses which Congress specifically charged NIAID to investigate and prevent, have mushroomed to afflict 54 percent of children, up from 12.8 percent when he took over NIAID in 1984.
One of the primary culprits for this change was the 1986 law with gave vaccine manufacturers immunity to injury lawsuits (incentivizing a flood of unsafe childhood vaccines to enter the market):
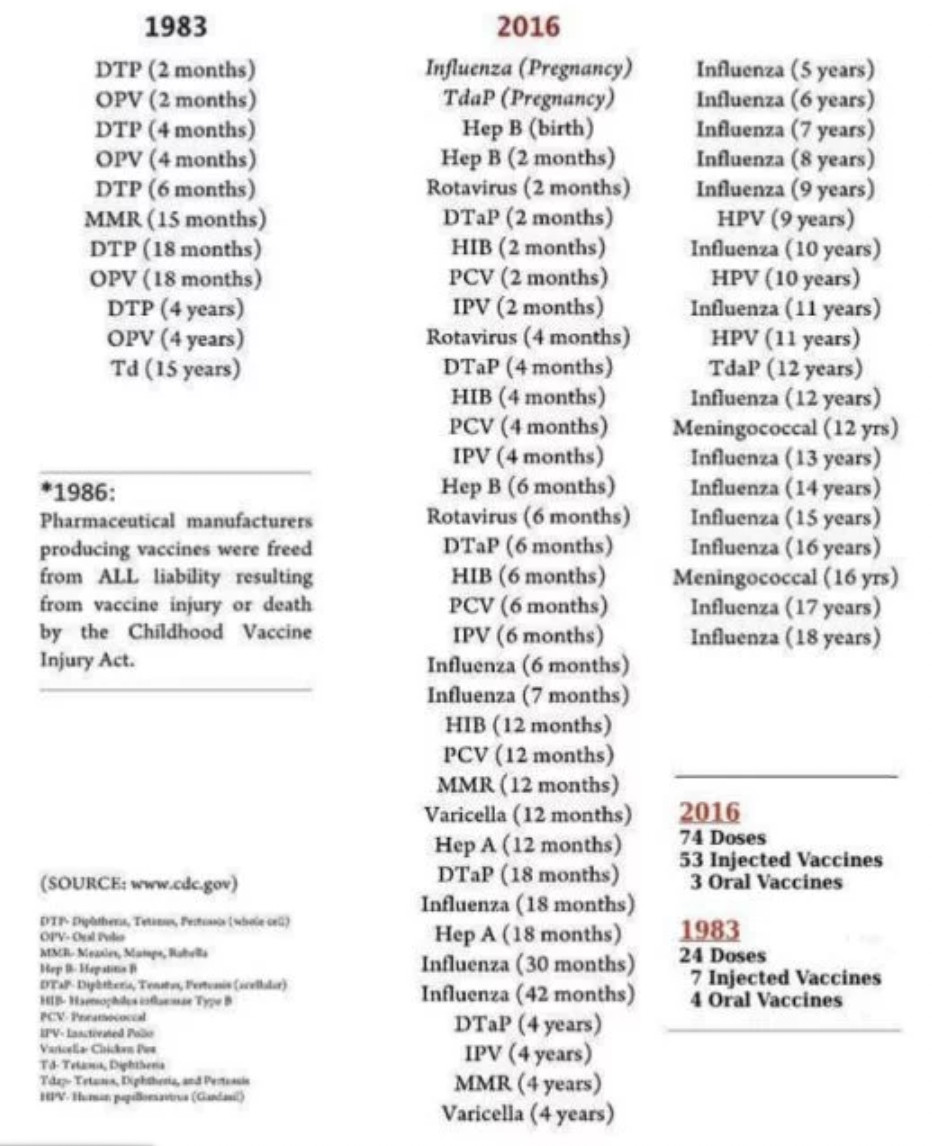
Note: the vaccine schedule has since been updated to include 2-3 COVID-19 vaccinations and an RSV vaccine.
This in turn touches upon a critical point. Much in the same way "autism is a spectrum," the injuries that follow from vaccination occur on a spectrum as well, and the autism spectrum comprises just one subset of them. For example:
•The processes I've discussed here, particularly an impaired zeta potential, also underly Alzheimer's disease—another disease that continues to increase despite decades of costly research that has thus far failed to find a solution.
• Large datasets have now shown the COVID vaccines are linked to brain fog and cognitive impairment (e.g., in individuals over 65, COVID vaccination increased the risk of mild cognitive impairment by 138% and the risk of Alzheimer's by 23%. After the COVID vaccines rolled out in the Netherlands, there was a 24% increase in doctor visits for memory and concentration problems in adults).
To recap:
1. Contrary to popular belief, there is actually a great deal of compelling evidence linking vaccines to autism.
2. There is presently no accepted explanation for what is causing the explosion of autism we are facing.
3. The only solution that's been offered for autism is more care services ( Peter Hotez even cites money being diverted from those care services into looking at the causes of autism as why it is so unconscionable for anyone to link vaccines to autism)—something that is not sustainable as the numbers of autistic children keep increasing.
4. The explosion of autism is one of the costliest diseases facing our country, so decades of hand waving that has insisted there's no scientifically valid explanation for this explosion simply doesn't cut it.
Fortunately, for the existing PR system to work, it has to have a monopoly on all sources of information so that its absurd narratives can always remain unchallenged. While that was long the case, over the last few years, that monopoly has broken, in part due to recent political shifts inviting widespread skepticism of the media (e.g., everyone being lied to about the COVID vaccines) and in part due to the internet more and more enabling the free diffusion of information.
That, in short, is why RFK Jr. is now able to conduct a real investigation into the causes of autism that should have been done decades ago but never was and why each of us must use our voice to make sure he is able to conduct that investigation.