By A Midwestern Doctor
The Forgotten Side of Medicine
September 30, 2025
Last week, President Trump was scheduled to give remarks on the potential causes of autism. Shortly beforehand, the press became aware Trump would focus on the link between Tylenol and autism (which some theorized was due to NIH scientists leaking that information), resulting in the national media collectively ridiculing that link immediately before the press conference. Possibly in response to this, the President then gave a very different press conference, which was arguably what the autism community has been waiting decades for.
Trump announces alleged link between Tylenol and autism during press conference
In that press conference, Trump stated:
• He had felt very strongly about bringing attention to vaccines and autism for 20 years and that solving this was more important to him than the economy (which is typically Trump's number one focus).
• He felt that we were giving too many shots too quickly and they needed to be spaced out (which is true, as severe vaccine injuries become increasingly likely the more closely and earlier vaccines are taken-but the medical field has refused to acknowledge this and reduce vaccine injuries as doing so would be akin to an admission vaccines are not "100% safe").
• He believed there was no reason to give the hepatitis B vaccine prior to children being 12 (which, as I showed here, is true).
• That Tylenol increases the risk of autism, so if possible, it should be avoided during pregnancy and you should not give it to infants.
Note: in addition to his public statements repeatedly linking vaccines to autism despite facing widespread criticism for them (e.g., consider Second Republican Primary Debate - Main Debate - September 16 2015 on CNN ), multiple associates of Trump's family have explained to me why Trump is personally invested in ending vaccine induced autism.
After which Secretary Kennedy stated:
Some 40 to 70% of mothers who have children with autism believe that their child was injured by a vaccine. President Trump believes that we should be listening to these mothers instead of gaslighting and marginalize them like prior administrations.
Some of our friends like to say that we should believe all women. Some of these same people have been silencing and demonizing these mothers for three decades because research on the potential link between autism and vaccines has been actively suppressed in the past. It will take time for an honest look at this topic by scientists.
As I heard this announcement, like many, I felt this was remarkable progress on a previously unsolvable issue. I was also grateful Trump drew mainstream attention to the concept it was not necessarily a good idea to "treat" an uncomfortable fever, and noted that his repeated statement that pregnant mothers should do their best to "tough it out" rather than take Tylenol was very similar to conversations I'd had throughout COVID with non-pregnant patients.
However, after I thought about it a bit more, I realized it might not have been a good decision on Trump's part to implore people to avoid taking something that was actually toxic.
The next day, to show they believed in Science, numerous pregnant mothers began posting videos of themselves taking large amounts of Tylenol (which I compiled on X here). These include a pregnant gynecologist training in fertility medicine showing off taking Tylenol, along with a nurse ( I've previously corresponded with) sharing the tragic story of a 23-25 week pregnant mother who'd done this and destroyed her liver.
These events, in short, highlight why there are serious but largely unaddressed issues with Tylenol.
Over the Counter Pain Management
Because of how uncomfortable pain is, pain treatments have long been a core market in medicine. Remarkably however, most of the standard pain therapies have serious issues and often progress patients to needing more and more severe interventions. Steroids, for example, have a myriad of often severe side effects, and when injected into joints, weaken the ligaments, hence providing temporary relief at the expense of the joint, which in turn causes the patient to eventually require a joint or spine surgery ( which often creates a host of permanent issues).
Typically, the first line treatment for pain is to get an over-the-counter pain medication, of which a few exist in the USA: acetaminophen (Tylenol), ibuprofen (e.g., Advil or Motrin), naproxen (e.g., Aleve or Naprosyn), aspirin or topical diclofenac (Voltaren gel). Unfortunately, these medications (with the possible exception of topical diclonfenac) all have a dose-dependent toxicity, and typically only elicit a partial improvement in pain. As such, patients frequently take additional doses to further reduce their pain which is often quite dangerous (or alternately, they overdose to commit suicide).
Many, in turn, consider NSAIDs (e.g., ibuprofen and naproxen along with stronger prescription NSAIDs) among the most hazardous drugs in the U.S. because:
- They are the leading cause of drug-related hospital admissions- often due to heart attacks, strokes, bleeding, and kidney failure (e.g., at least 107,000 Americans are admitted to hospitals each year for NSAID GI bleeds).
- Kidney damage is a significant risk. One study found a 20% increased risk of kidney disease from NSAIDs; others found up to 212%. Amongst kidney failure patients, 65.7% were found to be chronic NSAID users.
- NSAIDs raise cardiovascular risks. NSAIDS also increase the risk of heart attacks and death (e.g., extensive studies have found between a 24-326% increase 1, 2, 3). Two of the worst ones, Vioxx (Merck) and Celebrex (Pfizer), were designed to reduce stomach bleeding but instead caused heart attacks and strokes. Merck hid data on Vioxx's risks; eventually it was withdrawn after an estimated 120,000 deaths. Celebrex, still on the market, has been linked to 75,000 deaths. Merck's handling of Vioxx later informed how pharma pushed the HPV vaccine and mRNA vaccines.
- Gastrointestinal bleeding is common and often fatal. In 1999, over 16,000 Americans died from it. NSAIDs also cause small bowel damage in over 50% of chronic users-often undetected-leading to "small bowel enteropathy" and possibly chronic illness through gut permeability.
- They impair healing, especially of ligaments, creating long-term re-injury risk.
Trials alleging the benefit of NSAIDs are frequently intentionally deceptive and frequently create the illusion of a benefit where none exists. What this means is that many patients ruin their lives with drugs that did almost nothing for them in the first place.- Peter Gøtzsche
Unfortunately, NSAIDs remain amongst the most commonly prescribed drugs, and are frequently given for musculoskeletal injuries.
Note: the dangers of NSAIDs are discussed further here.
The poor efficacy of the OTC pain medications, along with their significant toxicity, in turn was one of the primary reasons I spent the last year of my life trying to bring attention to DMSO. This is because DMSO is dramatically more effective than any other over the counter option (e.g., I compiled a large volume of literature demonstrating that here, and I have now received well over a thousand reports from readers saying it produced miraculous improvements in pain)-essentially making it a crime a safe and affordable pain solution is not available to the public.
Lastly, since the current topic at hand is maternal safety during childbirth (where NSAIDs are strongly advised against due to a variety of issues they create for the fetus), many questions have been raised over if DMSO can be used instead. In turn, I have seen a lot of data suggesting DMSO is safe for the fetus (compiled here), seen numerous studies where pregnant mothers who received it had healthy children, and know the German DMSO community has not observed any issues from taking it while pregnant or while breastfeeding (whereas in contrast it has greatly helped developmentally delayed children). Likewise, we frequently use DMSO to treat mastitis while breastfeeding, and have not observed any issues from it.
Conversely, numerous reports show that if DMSO is injected directly into developing fetuses it causes birth defects (which is vastly different from the minute concentrations which will reach the fetus from topical applications), one study found that injecting pure DMSO into the abdomens of developing mice impaired neuronal development while a third found higher concentrations than achieved through topical applications impaired early neuronal development.
Given all of this, I think topical DMSO, when needed is most likely safe during pregnancy (or at least safer than the alternatives), but it has never been formally studied, as due to the politics surrounding thalidomide when DMSO was discovered, the DMSO field made a decision to simply never use it in pregnant women. That said, within the scientific literature, as far as I know, no cases of any toxicity to the offspring of animals from topical skin applications of DMSO to the pregnant mother have ever been reported.
Tylenol Toxicity
Tylenol (acetaminophen or paracetamol) is one of the few over-the-counter alternatives to NSAIDs and is generally considered safer than NSAIDs (making it frequently be a common alternative to them), though, it too, is often ineffective for severe pain. Still, while less toxic than NSAIDs, it carries a major risk-when metabolized, it has three different ways the liver can break it down, two of which are relatively harmless and one of which that produces the metabolite NAPQI (N-acetyl-p-benzoquinone imine) which is highly toxic to liver cells because it irreversibly binds to essential cellular proteins.
Typically, relatively little NAPQI is produced and quickly neutralized by liver glutathione. However when too much Tylenol is taken, the other detoxification pathways get saturated, shunting Tylenol metabolism to the NAPQI pathway, at which point the limited glutathione stores of the liver can get used up, and rapid liver death from unneutralized NAPQI ensues.
As a result, Tylenol overuse leads to 56,000 ER visits, 2,600 hospitalizations, and 500 deaths annually in America.
Note: certain conditions lower Tylenol's toxicity threshold and hence increase the likelihood of an overdose (e.g., chronic alcohol use, malnutrition, fasting, eating disorders, chronic liver disease, certain medications, older age, and genetic variability in liver metabolism).
Additionally, Tylenol also has a few other major issues:
• NAPQI is also toxic to the kidneys, and in 1-2% of overdose cases (with some sources saying 2-10%) the kidneys are also damaged. Within FAERS (which misses most reports), one study identified 1,288 reports of APAP-associated kidney injury, which disproportionately affected younger patients (and according to the study's methods, were 2.4 times more likely than ibuprofen to cause kidney injuries).
• Many studies associate gastrointestinal side effects with Tylenol use. In one review, their ranges were as follows: abdominal pain (3.9-5.4%), diarrhea (2.2-5.9%), dyspepsia (0.9-6.3%), nausea (1.5-5.4%), vomiting (1.6-1.6%). overall GI AEs (7.9-9.0%), medically significant GI AEs (5.3-5.3%), serious GI events requiring hospitalization (0.2-0.3%).
• In one review, Tylenol was found to increase the risk of the following conditions: bleeding or perforated peptic ulcers (+6-121%), uncomplicated peptic ulcers (+4-115%), lower GI bleed (+15-145%), heart failure (+9-98%), myocardial infarction (+0-73%), hypertension (+7-62%), chronic renal failure (+19-129%).
• A systematic review identified data suggesting chronic Tylenol use increased blood pressure (a 4mmHg rise in hypertensive patients), increased asthma (a possible 15% increase), caused a 3.6-3.7 increase in gastric bleeding (which increased further with concurrent NSAID use), and had a possible association with end stage kidney disease (being responsible for 10% of cases).
• Tylenol has been associated with an increased risk of blood cancers, +16% from low use and +84% from high use (with the increase being roughly double in women). Additionally, the following increases were seen with high use: myeloid neoplasms (+126%) plasma cell disorders (+142%), other mature B-Cell neoplasms (+81%)-with smaller increases being seen from lower doses.
• Tylenol has been associated with rashes and hypersensitivity reactions, has a required warning label for causing Steven-Johnson syndrome (a severe hypersensitive reaction where skin peels off), and in one review, was found to cause hypersensitivity reactions in 10.1% of children undergoing oral challenges.
• In children of mothers chronically using Tylenol, a review found the following increases: hyperkinetic disorder (+37%), ADHD medication use (+29%), autism spectrum disorder with hyperkinetic symptoms (+51%), asthma in offspring from frequent use in late pregnancy (+110%), asthma in offspring from any use during pregnancy (+15-17%), undescended testicles (with the greatest increased risk being seen if used for over 2 weeks in the second trimester).
Note: since vaccines cause fevers, many have pointed out it's possible some of the increase in neurodevelopmental disorders from Tylenol is actually due to maternal vaccinations taken during pregnancy.
• A recent systematic review of 46 studies which had been conducted on the risk of Tylenol during pregnancy causing neurodevelopmental disorders (NDDs) in offspring found the majority of studies detected an increased risk, that those of higher quality were much more likely to detect the association, and that the increase was dose dependent. The increased NDDs included autism, ADHD, and other NDDs affecting learning, social/motor skills, attention, cognition, emotions, and behavior.
Note: this study is arguably the most definitive proof Tylenol is not safe during pregnancy and was the one Trump and RFK's team highlighted at their recent vaccine announcement.
All of this led to a rather peculiar media phenomenon many online pointed out:
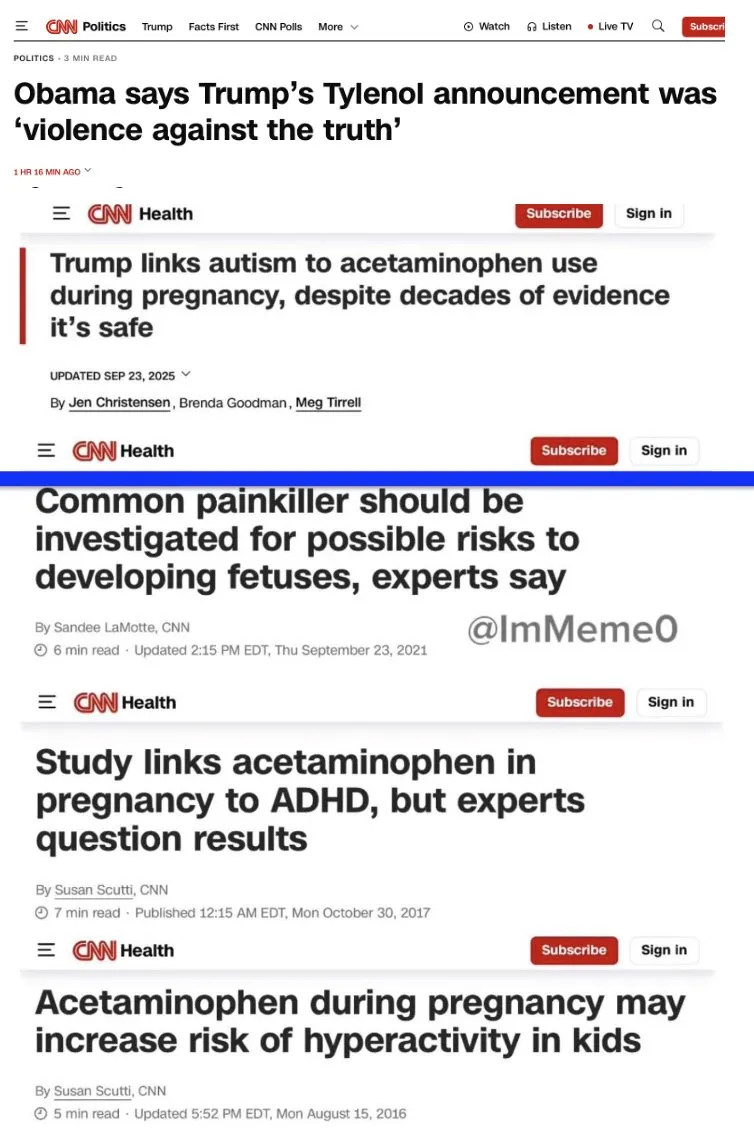
Note: numerous internal documents and public statements have shown that by 2017, Tylenol's manufacturer was well aware of the drug's link to autism. Additionally, while not highlighted by Trump, SSRI antidepressants have been observed to cause a variety of issues for the fetus (e.g., one review found an 82% increased risk of autism).
Treating Fevers
A standard procedure at hospitals to ensure nothing bad happens to patients is to have nurses check in on patients every few hours and to take their vital signs, then if anything is abnormal, contact the supervising doctor and ask them to do something to address the abnormality. Because of this, anyone who has worked in the hospitals has gotten a lot of calls from nurses to address fevers in patients and one of my continual challenges in that setting was telling the nurses I did not want to treat the fever—something which I found doctors had diametrically opposed views, with the majority of doctors I interacted with wanting to treat the fevers. Having put up with this for as long as I can remember, I hence was quite astonished to see the head of the FDA speak out against this practice:

Note: while the figures vary, the majority of studies I've found found the majority of doctors will treat fevers (e.g., one ICU study found 58%-70% of patients with fevers ≥38.0°C [100.4°F] were given Tylenol, 92.3% of surveyed doctors said they would treat fevers above ≥38.0°C, 84% of French doctors said they would treat childhood fevers, 30% of doctors said they would treat a childhood fever between 37.0°C to 38.0°C).
Why Do We Treat Fevers?
There are a few justifications for treating fevers:
1. Fevers significantly increase metabolic demand on the body, which places additional stress on vital organs by raising oxygen consumption, heart and respiratory rates, and energy expenditure. For this reason, in an ICU setting, where the functions of those organs is compromised, it is thought that reducing that metabolic demand will prolong a patient's survival but simultaneously it is also acknowledged that fevers aid in the elimination of infections. Presently, there is not a clear consensus within the critical care field as to how fevers in critically ill patients should be managed and I found significant variations on this question in the current resources I looked at.
Note: UVBI, a potent therapy for infectious diseases that also treats a variety of other conditions and often appears to "re-energize" the body, as a myriad of poorly functioning systems resume their normal function during a UVBI session. I mention this as one of the primary "side effects" of UVBI is that when it eliminates an infection it will often create a fever.
2. Once you have a high fever, it can cause brain damage, so a key goal is to prevent that from happening:
• Hyperpyrexia is defined as a medical emergency, which must be treated, and the threshold for it ranges from 105.8°F to 106.7°F (with the NIH using the lower value and the primary medical textbook using the higher value).
• According to Penn State, brain damage from a fever generally will not occur unless the fever is over 107.6°F.
Note: the body has a cut off to keep from fevers from going too high (e.g., i n the pre-antibiotic era, fevers were rarely observed to go above 106°) and while these high fevers are sometimes still seen in severe infections, they are typically observed in patients with brain hemorrhages (or from other brain issues like hypothalamic dysfunction).
3. In children, the threshold for potential brain injury is thought to be lower, which is why fevers above 104°F are often treated — though in some cases, even lower fevers also are often addressed. Furthermore, 24.0% of parents, 11.8% of nurses, and 7.2%, of doctors when surveyed expressed this concern about potential febrile brain injury—despite those associations having been long disproven.
4. If children have fevers (typically after vaccination or certain infections), these can sometimes lead to seizures. For this reason, many parents and certain doctors (including some in America), will aggressively treat the fevers with Tylenol (or another medication) to prevent the fever despite there being no evidence it helps (e.g., a 2017 Cochrane review found fever reducing medications provide no benefit for preventing febrile seizures and the American Academy of Pediatrics recommends against this practice).
5. To reduce the discomfort of the fever. This constitutes the primary reason most Tylenol is prescribed, and I suspect traces back to a need by medicine to be able to "do something" in the face of febrile illnesses (or the initial marketing campaign for aspirin—the first blockbuster drug in history). I do not agree with this approach.
Note: better pediatricians will counsel their patients to not give Tylenol to infants for minor discomfort and instead only advise using it if the infant is showing significant discomfort. However, parents will often immediately try to treat light fevers, as our culture has created the (erroneous) idea this should be done and benefits the infant (as fevers are "bad").
Conversely, the following arguments exist against treating fevers:
1. Fevers provide valuable diagnostic information (e.g., they can alert you to the presence of a new infection or the recurrence or exacerbation of an existing one), hence making it quite challenging to effectively manage patients if this signal is suppressed (particularly if the infection only causes low grade fevers and the patient is already being treated with immune suppressing drugs for an autoimmune condition).
Note: in infants, unexplained fevers over 100° often warrant a (justified) immediate evaluation for sepsis—which is one of many reasons why the (fever causing) newborn hepatitis B vaccine is so problematic.
2. Certain autoimmune and infectious diseases (e.g., Malaria) are characterized by relapsing fevers. For this reason, if a fever is suppressed artificially, that diagnostic signal is lost.
3. The body relies upon fevers to eliminate illness, so in theory suppressing fevers suppresses the body's ability to suppress illness. I am inclined to believe this is true (particularly given the cases I and others have observed). However, when I reviewed the literature which assessed this question, while it was observed in fully controlled trials where people were deliberately infected at the start ( e.g., with influenza), a 2023 systematic review of less controlled trials (many of which it stated had significant methodological issues) found there was no difference—suggesting this question still, quite remarkably, has not been adequately studied.
Note: that meta-analysis on fever suppressing medications only assessed the resolution of symptoms (e.g., fevers) rather than the actual elimination of infection.
4. As Tylenol has systemic toxicity and reduces liver function and glutathione (which is also necessary to detoxify toxins) this can potentially worsen certain illnesses. This, in turn, is why Tylenol is commonly believed to increase the likelihood vaccines will cause autism as it impairs the body's ability to detoxify the vaccine hence making it more vulnerable to those toxins.
Note: I recently learned through a reader that animal studies show Tylenol also depletes glutathione in the brain.
5. Suppressing febrile illnesses transforms them into more severe infections.
Of these, the fifth is the least appreciated and hence will be expanded upon.
The 1918 Influenza
In December of 2019, through internet forums, I became aware of COVID-19 and gradually became very worried it would hit the United States and cause a lot of problems due to it being an "incurable" illness (as there was a strong historical precedence how things like this played out). Because of that, we spent a lot of January and February trying to study the lessons from the 1918 pandemic (many of which formed my initial treatment protocols), and from the lessons I learned (along with those from many other sources), developed protocols that allowed people who otherwise would have likely been sent to a hospital (and die) to survive.
Note: I consider the 1918 influenza to be one of the most deadly and devastating pandemics in history (based on both reviewing the primary literature from the time and speaking to people directly connected to the events). For context, over 2.5% of those infected died (with much higher rates ranging from 12%-90% being seen in Native American populations)—a death toll which is unfathomable in the modern era.
Throughout that literature many of the clinicians treating the infection felt that it was a very bad idea to treat the fevers with aspirin, and again and again, they reported patients who'd previously been treated with aspirin had the poorest responses to the other therapies that typically worked to treat the illness.
Note: the 1918 influenza occurred the year after aspirin's patent expired, and during the pandemic, heavy doses (that were frequently toxic by modern standards) were routinely used. For this reason, many believe the overuse of aspirin was responsible for the severity of the pandemic. However, when I explored the primary literature of the time, while it was clear aspirin exacerbated cases, many accounts I came across made it clear aspirin could not be the sole culprit for the pandemic. Unfortunately, despite having looked at many different possibilities, I have still not been able to identify a definitive candidate.
Since that time, fevers have been shown to be critically important for fighting infections. Some of the key pathways which have been mapped out include:
•Fevers boost the activity of immune cells like neutrophils, monocytes, and T-cells, increasing their motility, phagocytosis, and production of reactive oxygen species.
•Fevers promote type I interferon responses that inhibit viral replication.
•Fevers trigger heat shock proteins to activate immune defenses and disrupt pathogen replication by damaging their proteins, lipids, and nucleic acids, especially at infection sites where temperatures can rise significantly.
•Fevers work synergistically with stressors like iron deprivation to amplify damage to pathogens, particularly rapidly dividing ones, and create an environment where fever-tolerant pathogens are outcompeted.
•Fevers slow pathogen growth early, helping to control infections and provide time for adaptive immune responses to develop.
Note: long before COVID, we had discovered one of the fastest ways to get over a viral illness was sometimes to heat the body up in a sauna.
Because of all of this, during COVID, I was acutely aware that it might not be a good idea to suppress fevers with Tylenol or ibuprofen. I then had multiple conversations with people out of the area where I advised them against doing this, but they did anyways (because they did not feel well) who then decompensated and had to go to the ER. Simultaneously, I ran into a few situations earlier in the pandemic where due to geographic isolation, no therapeutic option was available for the illness. As such, I tried using the same easily available approaches I'd read worked in the 1918 influenza, and frequently saw them significantly help.
Note: give or take everything tried during the 1918 influenza failed, hence making the occasional things which did work quite noteworthy to me.
From this process, I found that heating someone who was acutely ill (particularly infrared mats), beyond improving the course of the illness, would often make them immediately feel significantly better and no longer want a fever medication. From this (and noticing what I'd felt within my own body), I formed the hypothesis that the discomfort from fevers results not from the heat in the body, but rather the strain the body underwent from trying to heat itself. Unfortunately, since I only became aware of this during COVID, we've had limited time to validate this hypothesis, particularly since in more frail patients, there is an understandable hesitation to heat them as they may not be able to tolerate that (so we still do not know the safe or optimal way to do this).
Smallpox Vaccines
Many do not know the anti-vaccination movement originated with the smallpox vaccines or that this was a result of the vaccine frequently failing to prevent smallpox and severely injuring many recipients (detailed here).

When the smallpox vaccine was applied (by scraping it into an incision on the arm) it would frequently create a significant inflammatory skin reaction, and in time, the medical field observed that those who the vaccine failed to protect from smallpox had also not developed the characteristic skin eruption from vaccination. As such, the medical field adopted the stance that if the vaccine "did not take" it needed to be re-applied until the skin eruption happened so that the patient would develop immunity to smallpox.
In contrast, dissident physicians of the era (particularly those who had also trained in homeopathy) developed the perspective that:
•The skin reaction was a proxy for a functioning immune system and hence a pointless ritual as those vulnerable to smallpox in the first place were those in whom the vaccine would "not take."
Note: a case can be made this somewhat applies to other vaccines too (e.g., I discussed it with the newborn hepatitis B vaccine here, a pivotal study showed those who developed myocarditis from the vaccine could not develop neutralizing antibodies to the spike protein resulting in free spike throughout the blood stream, and it is well recognized some individuals do not develop titers from routine immunizations).
•At that time, patients began developing highly unusual neurological disorders following smallpox vaccination that had not been seen in the past, and again and again, it would be the case that the problematic smallpox vaccine "did not take." This led the authors of the time to conclude that the vaccine had "gone inward" and that rather than externally cause an unpleasant skin eruption, had instead caused a much worse chronic issue.
Lessons from Chinese Medicine
I view Chinese medicine as an incredible resource for understanding the medical history of humanity as the system was largely completed two thousand years ago, and a continuous written history exists since then (whereas our current form of medicine is very young). Because of this, it's possible to see how the changing health of humanity shifted that medical system, by noting how certain diagnoses became much rarer and inferring that indicated a shift in the disease patterns of humanity.
Since the concept of microclotting causing disease also exists within Chinese medicine (where it is called blood stasis), it caught my attention that many of the unusual neurological issues described from the smallpox vaccine mirrored those ascribed to blood stasis. Furthermore, within Chinese medicine, it has been a relatively recent shift in its 2000-year history that blood stasis came to be seen as a primary cause of illness, and that shift roughly coincides with when the smallpox vaccine (and smallpox variolation) was introduced to China.
Within Chinese medicine, there is a belief that the symptoms of a disease vary depending on how deeply they have penetrated into the body, and as such, different treatments are used depending on what stage the illness is at, with the therapeutic goal generally being to expel the pathogenic factor from the body. From having reviewed the descriptions of these stages, I believe that many reflect increasing microclotting in the body, as initially, systemic microclotting will only compromise the blood flow in the smallest vessels (which characterizes the superficial vessels), but as the electrical potential of the blood worsens, larger and larger clots form which become able to obstruct the medium sized vessels, and eventually the large ones.
Note: this was demonstrated in experimental monkeys who were allowed to have a malaria infection progress to being fatal (which was immediately preceded by the blood flow freezing in the largest vein of the body), and by the observation in critical care medicine, that, shortly before death, blood in those veins will become "echogenic" and possible to see on ultrasound due to large clumps of blood forming within the vena cava. 1, 2, 3
In turn, it's generally recognized that if the pathogenic factor is able to penetrate deeper into the body, if not lethal (which can happen) the condition transforms from an acute reaction, to an insidious "latent" chronic illness which gradually depletes the body and often becomes quite severe.
Because of this, the general viewpoint (which I also ascribe to) is that pathogenic factors should be identified and expelled (which amongst other things is what infrared saunas appear to do). However, one school of Chinese medicine which emerged in the 1600s during a period where plagues were routinely killing people instead adopted the opposite perspective.
That school suppressed the acute reactions to these illnesses, since the "heat" produced within the body during the acute reaction was often fatal (even when treated with existing Chinese medicine approaches), so they concluded the best option was to suppress the heat and wall it off within the body by turning it into a (pathologic) latent heat which could be dealt with later once the patient was no longer in danger of dying.
I mention this because while the scenario China faced in the 1600s is very rare now, I too have run into situations where I felt whatever issue was expressing itself was too much for the patient (or in a few cases myself) to handle, and reluctantly made the decision to suppress it and deal with the issue later when I felt it could be handled.
Note: this also sometimes came up with psychiatric issues.
Fevers and Cancer
As medical knowledge and science were rapidly evolving in the 1800s and early 1900s but the AMA's monopolization over medicine had not yet been established, a variety of medical systems emerged with unique insights that allowed them to provide enough benefits to patients they were able to persist despite countless attempts by the medical industry to eliminate all competition.
Anthroposophic medicine, for example, originated from the spiritual perceptions of an Austrian mystic, and remains widely used in certain circles (despite Rudolph Steiner having passed away a century ago in 1925).
One of the many perspectives Steiner held was that cancers were a result of a "cold" state where the warming influence of the body's bioenergetic field was diminished, leading to a lack of proper inflammatory activity and uncontrolled physical growth. Fevers, conversely, were seen as a necessary, health-promoting process where the spirit generates warmth (which is then transmitted through the brain and nervous system) to reorganize the body, potentially preventing conditions like cancer by maintaining bioenergetic vitality and immune strength. Put differently, Steiner correctly identified that the immune system was responsible for suppressing cancer before this concept was known by the medical field, and likewise that fevers are generated by the brain (hypothalamus) and then produced via the (sympathetic) nervous system.
Likewise, Steiner believed childhood illnesses which produced fevers (e.g., measles) were critical for allowing both the body and the immune system to mature, and that fevers made the body more malleable to the spirit reshaping it (thereby allowing the hereditary tendencies of the body to be overwritten and molded into what the spirit wished for the body).
Note: a significant portion of the water within the body exists in a gel-state where it behaves like a liquid crystal. Many within my circles believe trauma and various degrees of neurologic dysfunction are stored within malformed pockets of it (as agents like lidocaine which disperse it frequently produce great benefit when applied to pockets of stagnation). Many others have proposed that since the fraction of water existing in the gel state decreases with increasing temperature, fevers function to temporarily disperse liquid crystalline water, thereby giving the immune system more access to tissue and a way for cells to detoxify by purging metabolic waste products (a theory the leading researcher in this field has stated he thinks is likely true but currently unknowable due to the difficulty in modeling it). Assuming this is true, this could potentially explain Steiner's belief that fevers increase the malleability of the body.
Since Steiner's time, evidence has accumulated supporting his hypothesis, with numerous studies finding:
•Not having a childhood chickenpox infection increasing your risk of brain cancer later in life. 1, 2, 3, 4
•Not having a mumps infection increasing your risk of (frequently deadly) ovarian cancer. 1, 2, 3
•Previous infections of influenza, measles, mumps or chickenpox were found to decrease one's risk of malignant melanoma.
•Other cancer studies have found similar results. 1, 2
•Measles and mumps have also been observed to nearly halve the likelihood of having a heart attack, stroke, or brain bleed.
Note: a case can hence be made, that even assuming vaccines were 100% safe and effective (which they aren't), the severe diseases prevented by having these infections outweigh the benefits of preventing the harm the infections can cause.
In tandem with Steiner's perspective, in 1891, an American surgeon observed that a patient with an inoperable sarcoma experienced spontaneous tumor regression after surviving a severe streptococcal infection (erysipelas). From this, he concluded that the high fever may have cured their cancer, and over the next few years created a mixture of Streptococcus pyogenes and Serratia marcescens endotoxins, which successfully treated a large number of cancer patients and began having purified versions of his toxins produced by a few pharmaceutical companies.
However, as time moved forward, the newly emerging science of radiation and chemotherapy was viewed as a more reliable and predictable way to treat cancers (displacing Coley's toxins), and once he died in 1936, his approach became largely forgotten, culminating in the 1960s, where it, (like many other successful cancer therapies) was labeled as an "unproven cancer remedy" and consigned to the dustbins of history.
However:
•While Coley's toxins are not used, many new cancer "immunotherapies" (which are routinely used) were inspired by the toxins.
•A small contingent of alternative medical practitioners have continued using Coley's toxins with success for certain cancers.
•A related approach, whole body hyperthermia, directly heats the body up with an external source of heat in a controlled way. It has been widely used in Germany for decades, and the success of the approach has led to it having some acceptance in the broader oncology field where it is viewed as a potentially viable treatment for certain cancers.
Systemic Suppression
Over the years, many natural healers have shared with me their belief that healing requires moving deep issues to the surface, and that one of the major reasons why the conventional medical approach creates chronic illness is because the medications are suppressive and cause minor acute reactions to be transformed into much greater issues later on.
Note: most of the people espousing this viewpoint were homeopaths (in part due to homeopathy frequently requiring taking extensive case histories of patients, hence making it possible to detect these patterns). While it mirrors Chinese medical philosophy, as best as I can gather, the two originated independently. For example, the way homeopathy maps this process out ( Hering's Law of Cure) states that during treatment, symptoms improve from the head down, from the inside out (with the most important organs improved first), and in the reverse order in which symptoms emerged—which has parallels to but is not the same as how Chinese medicine describes it—suggesting both systems were simply doing their best to model a naturally occurring process.
In turn, they argued again and again, you could see cases where the chronic illness was preceded by the inappropriate use of suppressive medicines, and I lent a degree of weight to their observations as many of these people had been able to treat challenging illnesses conventional approaches had failed to help. Likewise, in my own experience I saw numerous cases where a confusing acute illness became a much more severe illness (and sometimes a lifelong incapacitating one) after steroids were reflexively given to address the acute symptoms (e.g., I have three friends who had perplexing symptoms from undiagnosed Lyme disease who became much, much, worse after steroids).
Note: as I discuss here, many superficial networks of vessels exist in the skin. I strongly suspect those transporting interstitial fluid, when partially obstructed, give rise to a variety of inflammatory skin disorders (as DMSO eliminates this stagnation and greatly improves many skin disorders), while when fully obstructed, the toxins they would transport and expel through the skin instead remain trapped deeper inside the body, and give rise to chronic illness. Given this, I've long wondered if steroids "work" by cutting off the superficial interstitial circulation.
Furthermore, many who ascribed to this philosophy believed that a parallel depth existed within the body, mind, and spirit, and that some illnesses which expressed themselves through physical symptoms originated from either the mind or spirit, so when suppressed physically (or psychiatrically) more profound issues would emerge in the mind or spirit.
Note: antidepressants have a variety of issues and create a variety of different characteristic responses. One common response is that they anesthetize one's emotions so that they both lose the joy in being alive and become able to tolerate extremely uncomfortable situations (e.g., an abusive job or relationship). Many have reported that the emotional suppression these drugs create caused them to waste years of their life in a bad situation they walked through in a waking daze, and that problematic spiritual disconnections often accompanied this. Likewise, I've also spoken with many people who were having powerful (but destabilizing) spiritual experiences that were addressed by psychiatric medications or institutionalizations, after which the spiritual components simply became more intense and destabilizing—many of which were similar to what an African shaman visiting American psychiatric institutions also observed.
In turn, I've never forgotten a conference which happened in the 1970s (I believe it was in 1974) where one of the world's leading homeopaths convened a panel to discuss what the likely consequences would be in the upcoming decades of conventional medicine routinely suppressing symptoms (e.g., it aggressively treating all fevers with medications and preventing the childhood febrile illnesses with vaccination).
At that conference, building upon Hering's Law of Cure (along with the recent mass introduction of suppressive steroids), they predicted that if conventional medicine continued to proliferate in its mass suppression of symptoms, in the decades to follow, we would see:
•We would see a global shift from less severe illnesses to more severe ones (e.g., cancers).
•That this suppression would cause physical illnesses to be pushed deeper into the body and be replaced with psychiatric illnesses, and in time spiritual ones (particularly when the psychiatric illnesses were also suppressed with medications).
Note: the predicted psychiatric illnesses included common ones (e.g., anxiety along with depression, which at the time was rarely an issue), psychopathy, mass shootings, self-harm and self-mutilation, and the public becoming willing to do crazier and crazier things. The spiritual ailments, included people wanting to be robotic rather than spiritually connected to life, and people knowing they were spiritually adrift because they'd lost their connection to life (which otherwise would have prevented much of this dysfunctional behavior).
It was hence quite noteworthy to me that many of these shifts indeed happened, and likewise to compare just how different patients in the 1970s (especially older ones) were. However, I also feel a very strong (albeit retrospective) case can be made that the increasing proliferation of vaccinations explains this shift.
Note: over the last 150 years, there has been a large decline in the general vitality of the human species (resulting in them becoming gradually sicker, less responsive to treatments, and less able to fight off chronic disease)—something I believe started around the same time the smallpox vaccines. Vaccination, suppressive medications, and the loss of the ability of humans to mount fevers are often cited as potential causes of this decline—making it noteworthy that the average body temperature over the last century has declined by approximately 1 degree (Fahrenheit).
Suppressive Antibiotics
While steroids are one of the medications most associated with "suppressing" illness, many others are too. For example, for years, many natural medicine practitioners (e.g., homeopaths) also told me they'd frequently seen antibiotics "treat" an acute infection but turn it into a chronic one. I wasn't sure what to make of this (as microbiome disruption could partially but not fully explain it) then discovered something similar existed in Chinese Medicine::
The concept of Latent Heat is very old in Chinese medicine, having been mentioned for the first time in the 'Yellow Emperor's Classic of Internal Medicine'. Latent Heat occurs when an external pathogenic factor penetrates the body without causing apparent symptoms at the time; the pathogenic factor penetrates into the Interior, and 'incubates' there, turning into interior Heat. This Heat later emerges with acute symptoms of Heat: when it emerges, it is called Latent Heat.
Note: in modern Chinese Medicine, antibiotics and vaccines are now proposed as sources of latent heat.
Much later, when I read Cell Wall Deficient Forms: Stealth Pathogens all of this finally made sense. This book argued that when bacteria are exposed to lethal stressors, particularly cell wall destroying antibiotics, while most will die, some will instead enter a primitive survival mode and transform into misshapen cell wall deficient (CWD) "mycoplasma like" bacteria which can radically change their size or morphology (and hence look very different). While these bacteria are hard to detect (and when seen, due to no one knowing they "exist," often mistaken for cellular debris and ignored), with the correct techniques they can be detected. In turn, the book provides a wealth of evidence that CWD bacteria:
•Are found within many "aseptic" tissues undergoing an autoimmune attack, with specific CWD bacteria associated with many different autoimmune disorders which have no known cause.
•Once the environment is "safe" can transform back into their normal form and cause a sudden recurrence of an infection—suggesting chronic infections are due to antibiotics creating a dormant CWD population rather than continual reinfection.
Note: many popular alternative schools of medicine (e.g., those of Rife, Naessens, and Enderlein) came from microscopes which could directly observe these pleomorphic bacteria continually shifting into new morphologies, and that disease states (e.g., cancer) correlated to specific morphologies, while other morphologies resulted in a symbiotic state of health (e.g., this is a video of the organisms Naessens observed). Since the morphologies adopted correlated with the internal state of the body, this gave rise to the belief that treatments should aim to create "healthy terrains" within the body, which would give rise to non-pathogenic forms of the bacteria rather than using antibiotics that provoked pathogen transformation.
Since becoming aware of this concept, I've run into numerous cases where it appeared to be the key issue and concluded certain chronic illnesses assumed to result from a gut microbiome disruption (due to antibiotics eliminating one strain of bacteria and allowing a more pathogenic one to take over the gut), were actually due to existing microorganisms being transformed to a pathogenic state. In turn, I am often mindful of which antibiotic is given (to avoid this happening) and simultaneously have seen many cases where undoing this pathologic transformation was necessary to address a chronic health issue.
Autism and Tylenol
During my first pediatric clinical rotation in medical school, I saw multiple cases where a child had a (relatively minor) reaction to a vaccine such as a fever and inconsolable crying for which they were given Tylenol, after which the fever disappeared but was replaced with a more severe reaction (e.g., a severe rash covering the body), with the parent frequently noticing the severe symptom immediately followed the fever disappearing, and sometimes stating the infant became more quiet prior to the severe illness onset.
Remembering what my mentors had told me about the importance of not suppressing fevers, I started exploring this question and over the years learned that many parents across the world (including many I got to know) had reported that a rapid developmental regression followed a fever being suppressed. As I never saw this in the pediatric patients I directly followed during any of the rotations during my medical education (and never gave vaccines once I completed my training), I assumed the severe regressions (including those leading to autism) were the same process I'd witnessed during my training, but a significantly rarer complication of suppressing fevers (as severe reactions tend to be rarer than more mild ones).
In turn, my focus naturally shifted to why, from which I concluded:
•This could be a direct illustration of the dangers of suppressing symptoms described through natural medicine.
•Fevers significantly increase blood circulation and reduce blood cell clumping, so they may be an adaptive process that partly prevents the brain damage vaccine induced microstrokes cause (hence making damaging microstrokes result from the fever being suppressed).
•The body's reduced ability to eliminate toxins (due to an excessive amount of gel-state water within it), and the liver's inability to neutralize the toxins (due to the stress Tylenol places upon it), made the toxins within the vaccine much more likely to cause harm.
However, I could see no way to definitively conclude which process was at work, so for that reason, here I tried to lay out the entire thought process behind each possibility. Likewise, while I mostly avoid it, there are certain circumstances where fever suppression is merited, and hence I've done my best to present both sides of the debate here.
Your support makes The Forgotten Side of Medicine possible. To receive new posts and support my work, please consider becoming a free or paid subscriber!
Reversing Suppression
Due to my concerns about COVID that began in 2019, I have explored more treatments than I can count for it, and now know well over a dozen which I've directly seen improve or resolve the illness—hence making it incredibly frustrating every alternative was suppressed to push remdesivir upon the country.
Even more frustrating, I found that most of these treatments worked the best when given in the early stages of the illness before severe symptoms had onset—yet the standard ER management for COVID was to simply give a patient Tylenol, send them home and tell them to come back if they became severe ill and needed to be hospitalized.
The abysmal failure of that approach (e.g., America spent the most on COVID yet had one of the highest death rates from it) illustrates that it is critical to re-evaluate how we treat infectious diseases—something I am quite hopeful for due to the unique influence MAHA, and its members like the FDA director, now has over American medicine.
In the final part of this article, I will review some of the common approaches we use to treat infectious illnesses that avoid the issues seen with suppressive medications (e.g., which antibiotics have the best risk-benefit ratios and which approaches provide the best results for treating viral illnesses) along with discussing some of the approaches I've seen reverse the effects of systemic suppression upon the body.