By A Midwestern Doctor
The Forgotten Side of Medicine
December 26, 2024
Recently, new data emerged showing that the COVID vaccines persist for up to 700 days within patients (and likely longer). As this is quite concerning to many, I was requested to write an article explaining how this happens, and how it relates to the egregious production process that characterized the COVID-19 vaccines.
Upsides and Downsides
A lot of things in life are trade-offs, and as I've gotten older, more and more I've come to appreciate how many things in our society boil down to the fact that the options for addressing them all have significant downsides, so in many cases no solution exists which is satisfactory to all parties involved.
As such, this dilemma is typically managed by some combination of the following:
•Having a biased focus which emphasizes the benefits of an approach a side supports and downplays its downsides (or conversely disproportionately focuses on the downsides of an opposing position). To this point, I've had countless issues I've debated both sides of and been able to effectively persuade audiences of each one-which highlights how subjective many of the entrenched beliefs we hold actually are (and, in turn, is why I put so much work here into fairly presenting both sides of each controversial topic I cover).
•Sweeping the downsides under the rug and gaslighting the populace into believing they don't exist.
•Blitzing the public into supporting a questionable policy before they have time to recognize its downsides, and if that fails, overtly forcing them to go along with it.
Note: I believe one of the reasons why governments frequently do horrible things to their people is because they are put in the position of having to "solve" a problem (but with no truly satisfactory way to do it), so they become habituated to using the three previous strategies to push their chosen policies along and simultaneously develop a collective mentality that those questionable approaches are necessary for the "greater good."
There are many different manifestations of this dilemma, many of which I believe are essentially reflective of a foundational concept in medicine-sensitivity and specificity.
An ideal diagnostic test would catch every instance of a disease (100% sensitivity) and simultaneously never have a false positive (100% specificity). Unfortunately, in almost all cases, this is impossible to do, and instead a trade-off exists where you can either prioritize sensitivity (which leads to a significant number of false positives) or prioritize specificity (which leads to a significant number of false negatives). During COVID for example, a decision was made to prioritize sensitivity with the PCR tests (by having a high replication cycle thresholds) so no cases of COVID would be missed, but this resulted in such poor specificity that the PCR tests effectively became worthless (except for drumming up fear) since they produced so many false positives.
As such, when tests are designed, attempts are made to ensure there is a good balance between sensitivity and specificity. In some cases this is successful (e.g., there are many lab results we will take at face value), but in many other cases, given the technology involved, it's not really possible to do so (or it is, but lobbying led to overdiagnosis so a medical product could be sold).
Similarly:
•Many policies in the justice system aims to enact fall into this same situation. For example, an ideal death penalty is robust enough to deter murder (and keep violent criminals away from the public), but simultaneously lenient enough that it doesn't accidentally execute innocent individuals. Since there is no way to have both perfect sensitivity and specificity on this, different states take radically different approaches to how they enforce the death penalty (lying all along the spectrum between sensitivity and specificity). Likewise, our judicial system was founded under the principle "innocent until proven guilty" whereas many other countries have judicial systems that are the exact opposite.
•In medicine, one of the greatest challenges is finding the appropriate dose, as people differ, so what might be a safe and therapeutic dose for one person could be toxic for another. As such, standardized doses are typically chosen by finding the best overall balance between efficacy (a sufficient dose) and safety (avoiding a toxic dose), but for many drugs, the standardized dose leads to many more sensitive patients becoming severely injured by the drugs (which is then commonly "addressed" by gaslighting those injured patients).
Note: a much more detailed discussion on the art of dosing can be found here.
•Every medical intervention has its risks and benefits, and ideally, the job of a physician should be to accurately weigh those to determine the best treatment for a patient (while simultaneously conveying what they are to the patient). Unfortunately, in many cases, they don't (which is a large part of why patients are so dissatisfied with the medical system).
Overall, there are three key takeaways from this paradigm I wish to focus on in this article:
1. It is often incredibly difficult to find an acceptable balance between sensitivity and specificity, and many of the conventions our society now follows were the result of years of debate and protest from both sides to find a palatable middle ground between the two.
2. In almost any sphere I frequently find rushed attempts to find an acceptable balance between two conflicting positions to be immensely flawed and prone to creating significant issues in the future.
3. Many of the issues with the vaccine program are encapsulated by this framework.
How Vaccines "Work"
Note: many believe the immune system is one of the least understood parts of physiology, something I would argue is a result of immunological research being focused on making profitable pharmaceuticals (e.g., vaccines) rather than understanding how it works.
In the classical conception of immunity, there are two types, innate immunity and adaptive immunity, with the innate response being relatively nonspecific (so it can work against a wide variety of infectious threats, including those the body has never seen before) and the adaptive one, which is uniquely suited to eliminating the specific invading organism.
The most widely accepted explanation for how the adaptive immune system works is " clonal selection theory" which states that the immune system:
1. Uses a random generation process to create a vast pool of potential antigen matching sequences.
2. Has vast number of different immune cells that each have those sequences attached to them circulate the blood stream.
3. Waits for one of those immune cells to contact an invading pathogen that the sequence it carries matches.
4. Have each of the immune cells be programmed to start rapidly reproducing once they get a sequence match.
5. Through the previous 4 steps, make it possible to produce a large number of immune cells which are specific to an invading organism (because they can bind to their antigens and alert the rest of the immune system to the organism's presence), and thus effectively neutralize the infection.
6. Once the process is complete, to leave behind memory B cells, which match the invading pathogen and are able to stimulate the immune response in a much more rapid fashion (thereby shortening the time that steps 3 and 4 take).

The theory behind vaccination is that if the specific immune response and memory B cells can be created before the body encounters a dangerous microbe, this can:
•Allow the body to mount a robust immune response before a harmful invading organism has time to multiply within the body and cause significant damage.
•Cause individuals to rapidly clear infections (rather than needing to wait for the adaptive response to kick in), thereby reducing or eliminating the amount of time they can spread the disease into the population.
•Cause individuals to develop an immune response at the site of infection (e.g., the membranes of the nose and throat), thereby preventing the organism from being able to colonize those areas and thus preventing its transmission.
Being able to do this is hence immensely appealing to governments, as it allows a single intervention (the vaccine) which can easily be distributed to everyone in a top-down manner (which is what governments are good at doing) to address a longstanding problem (infectious disease outbreaks) and more importantly, to allow the government to present the appearance of working in earnest to safeguard the public's health. Because of this appeal, throughout history, governments will get deeply invested in vaccine programs, and then once issues arise with those programs, double-down on the vaccine (e.g., with mandates) rather than reconsider the wisdom of the vaccine program.
Note: in a previous article, I showed how this misguided and tyrannical conduct has existed ever since the first vaccine (smallpox).
Vaccine Production
To "work" vaccines aim to mass produce a dangerous organism's antigen without the organism itself being present and then administer that antigen into the body. By doing so, the intermediate stage of an infection (where the organism has already reproduced enough inside its host to have a large number of antigens be available to match a circulating immune cell) can be achieved without the individual being in danger of being damaged or overwhelmed by the infection.
Unfortunately, unlike chemicals which can be rapidly synthesized, antigens are complex enough that they can only be produced by biological systems. As such, to produce the antigen, one of the following is typically done.
•Mass produce the infectious organism, then "kill" it so that its antigens can be collected, but the organism itself is not able to cause infections.
•Genetically modify another organism to mass produce a desired antigen, then kill it and extract the antigen (e.g. the HPV vaccine does this with modified yeasts).
•Modify the live pathogen (typically a virus) so that it can still cause the infection and reproduce inside the recipient but simultaneously is "weakened" so that it is less likely to cause illness.
•Genetically modify a "benign" virus to contain the antigen but be unable to replicate in the human body, then mass produce it outside the body, and have the body develop an immune response to the virus and the antigen on it once it is injected.
•Introduce mRNA into cells so human cells can produce large amounts of the desired antigen, which the immune system then sees (e.g., on the surface of the cells) and develops an immune response to.
The basic problem is that none of these approaches are perfect, and each has both its ups and downsides. For example:
•Most can create autoimmunity.
•In those where only a single antigen is used (and the virus spreads from human to human), if the vaccine actually works, it rapidly stop working because the pathogen quickly evolves a new antigen that no longer matches the vaccine.
•It contrast, the multi-antigen ones (which don't have that issue) are typically live attenuated vaccines, which then can cause those with weakened immune systems to develop infections from the vaccine itself (e.g., this happens with the polio vaccine-which is why the primary cause of polio now is from the vaccines rather than natural infections, but also can happen with others like the shingles and measles vaccine).
Furthermore, some infectious diseases respond fairly well to vaccination, but the majority do not, so at this point, the vaccine industry has already picked all the "low-hanging fruit" and hence faces an existential struggle to develop new proprietary (patentable) vaccines it can bring to market. For example, had it not been for COVID-19 (SARS-CoV-2), a SARS vaccine would have never been brought to market as it was well recognized the SARS virus was poorly suited for vaccination (which what we then saw throughout the pandemic).
Finally. even if a vaccine "works" it still has to be manufactured, and there are numerous cases of the tradeoffs being made resulting in a disaster. For example:
•To make the inactivated polio vaccine, the live polio virus had to be exposed to formaldehyde. However, the challenge with this was that if too much formaldehyde was used, it would damage the antigens on polio to the point they no longer matched those on the poliovirus, whereas if too little was used, some of the polioviruses would remain active and could then give the vaccine recipient polio. The creator of the vaccine (Salk) opted to prioritize efficacy over safety, which the government in turn supported, even when one of their own scientists (Bernice Eddy) warned them against releasing the vaccine (as it caused polio in her lab). That 1955 vaccine then infected at least 220,000 people with live polio virus in Cutter's vaccine, of whom 70,000 developed muscle weakness, 164 were severely paralyzed, and 10 died.
Note: an identical issue had happened on a smaller scale (9000 infections, 12 severe cases, 6 deaths) in 1935 with an earlier version of the inactivated polio vaccine. Likewise, (as I showed here) there have been dozens of incidents where an insufficiently inactivated or attenuated diphtheria, rabies or yellow fever vaccines severely injured hundreds of people (as the attenuated vaccines faced a similar issue with it being easy to over or under attenuate).
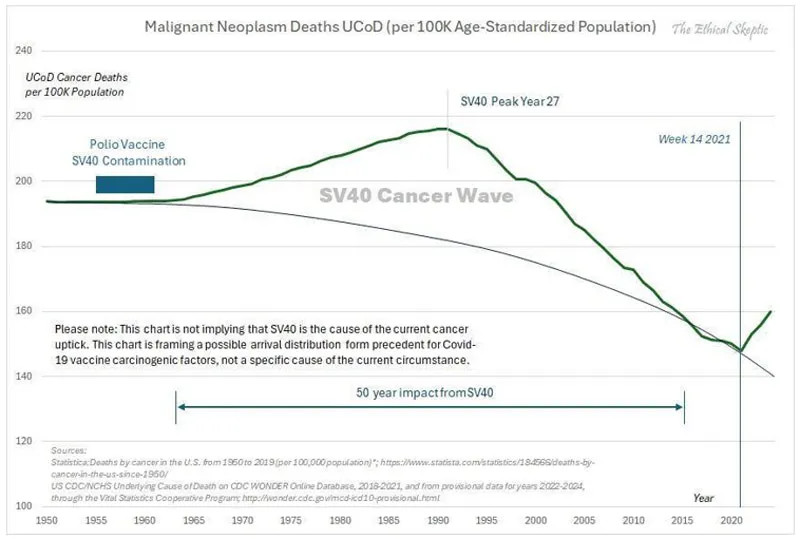
•Growing viruses for vaccines requires having a cell culture to grow them in. Monkey kidney cells were chosen because they worked well for doing this, but unfortunately were contaminated with the cancer causing SV40 virus. In 1962, Eddy again warned the government about the vaccine, but they still chose to give it to the public (and retaliated against her for speaking out), which in turn led to a wave of cancer sweeping through America, which until the COVID-19 vaccines was unprecedented:
Note: many other viral vaccines (particularly the live ones) also have had harmful viral contaminants identified within them, but unlike SV40, that contamination has not been acknowledged. Most noteably, a strong case can be made that HIV emerged from virally contaminated vaccines (that had been grown in monkey tissues).
•After a potentially dangerous strain of influenza (due to it having similarities to the 1918 influenza) was identified, a rush began to make an emergency vaccine for it (despite the FDA's chief influenza expert Morris accurately warning that strain posed no risk to America). Since it took a while to cultivate the virus for a live attenuated vaccine, in order to make the vaccine be produced fast enough to hit the market before the influenza strain disappeared, a decision was made to hybridize it with the PR8 strain, a fast growing influenza strain directly descended from the 1918 influenza. Morris warned against doing this, but was ignored ( and fired). That 1976 vaccine subsequently injured a large number of people (including some of our patients) and was a publicity disaster for the US government.
• The anthrax vaccine used during (and after) the Gulf War required growing large amounts of the bacteria, killing them, and then filtering out the most toxic components from the final vaccine preparation. The issue the manufacturer ran into was that because of how dirty the vaccine was, its contaminants clogged the filters the manufacturer used, so "solve" the problem and be able to manufacture the vaccine at scale for the military, the manufacturer opted to use larger filters which did not clog, but also didn't filter many of the toxic components out of the final products-which resulted in one of the most harmful vaccines in history being unleashed upon our military.
•Due to the challenges in producing it, the DTP vaccine (another killed bacterial vaccine) was notorious for having hot lots that killed their recipients (or left them with brain damage). In fact, one FDA pertussis specialist in 1976 stated:
Pertussis vaccine is one of the more troublesome products to produce and assay. As an example of this, pertussis vaccine has one of the highest failure rates of all products submitted to the Bureau of Biologies for testing and release. Approximately 15-20 percent of all lots which pass the manufacturer's tests fail to pass the Bureau's tests.
Eventually, the injuries that vaccine created led to so many lawsuits that the manufactures could not afford to continue producing the vaccine, at which point, the 1986 Vaccine Injury Act was passed. This shielded the manufactures from all future liability from it (hence allowing them to stay in business), and eventually incentivized the production of a safer but more costly pertussis vaccine.
•Frequently when an antigen is produced, it cannot solicit a sufficient immune response (unless a lot of it is used-which frequently makes the vaccine too costly to produce). To solve this problem, cheap (and toxic) adjuvants which enhance the immune response to the antigen are used, thereby allowing an affordable amount of antigen to be required for the final product. When the HPV vaccine was developed, it was discovered that its antigen (along with standard adjuvants) could not mount a sufficient immune response to get FDA approval, so a decision was made to use an experimental (but much stronger adjuvant) which worked-but also gave a large number of recipients autoimmune disorders ( at least 2.3%). Nonetheless, that trade-off was also accepted to get it to market.
In short, if you look at all these cases, a consistent pattern should be clear. Whenever there is a choice between getting a dangerous vaccine to market or holding off because there isn't a way to do it safely, the vaccine industry will always do the risky approach (especially in "emergency" situations) as they know they can unconditionally rely upon the US government to promote the product as "safe and effective" and then legally shield them from the disaster which inevitably follows.