By A Midwestern Doctor
The Forgotten Side of Medicine
May 6, 2025
Note: one of my favorite things about publishing on Substack is that I can continually revise articles as I learn new information (e.g., much has been added to the existing DMSO articles). As such, I periodically republish revised versions of the articles readers here found to be the most helpful and it is my aim to eventually unmask each of the commonly prescribed drugs that cause a lot of problems.
The years I have spent studying the medical industry have made me appreciate how often economic principles can allow one to understand its complex and contradictory behavior. For example, I believe many of the inconsistencies in medical ethics (e.g., "mothers have an absolute right to abort their children" and "mothers cannot refuse to vaccinate their children because it endangers their child's life") can be explained by simply acknowledging that whatever makes money is deemed "ethical."
Sales Funnels
In my eyes, one of the most important business principles for understanding medicine are sales funnels, a method of selling products where you initially cast a wide net, and then successively cast smaller nets for increasingly expensive products after catching your initial customers.
Note: the term "funnels" is used to describe how the sales pipeline gets narrower as you move to more expensive products.
I typically see two types of (often overlapping) sales funnels in medicine.
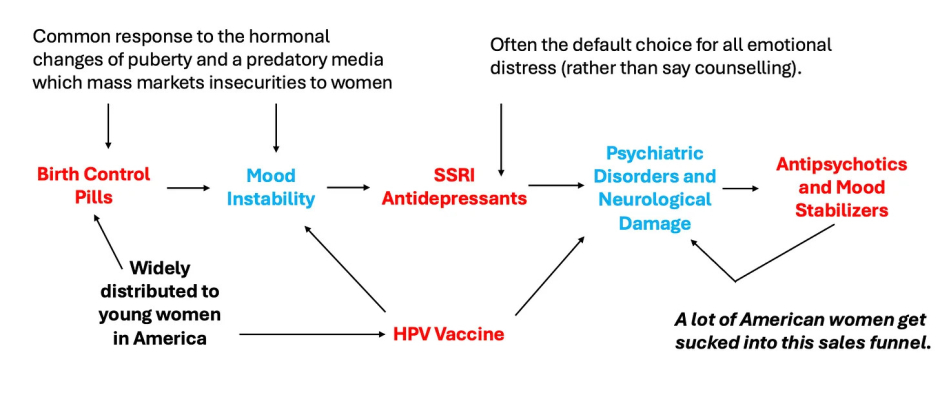
The first works by normalizing giving an "innocuous" drug to broad swathes of people and then selling increasingly expensive pharmaceutical drugs to treat the complications many experience from those drugs. One of the most insidious ones affects many of our girls and is one I've repeatedly tried to draw attention to:
Note: a good case can be made that many of the chronic illnesses our children suffer from now (which are very lucrative to "treat") are a direct consequence of the ever increasing number of vaccines in the marketplace.
The second funnel works by recasting "preventative medicine" and "promoting health" as the task of screening for each person for conditions they are at risk for. The results from these universal screenings are then used to justify selling them medical services (e.g., drug prescriptions). Once that screening becomes normalized, the industry will then pivot to expanding the funnel and having far more services be sold. For example:
•What constitutes a "safe" blood pressure has been continually lowered, and as a result, more and more people are put on blood pressure medications. This in turn has created a variety of problems (discussed further here). For example, the elderly (due to the arteries calcifying with age) need a higher blood pressure for blood to reach the brain, and many hence suffer lightheadedness and catastrophic falls from their blood pressure being lowered.
•Since we started mass cholesterol screenings, what constitutes a "safe" cholesterol has also been continually lowered by the corrupt committees who create the guidelines doctors follow to practice medicine. For example, a widely used calculator which determines ones risk of a stroke or heart attack consistently concludes people are at a high risk of a heart attack and must urgently start statins, yet almost no doctor in practice knows that a 2016 study of 307,591 Americans discovered the calculator overestimates their risk by 5-6 times. Similarly, most doctors aren't aware that beyond failing to benefit patients (in contrast to natural therapies which do improve heart disease), statins are also immensely dangerous drugs (discussed further here).
Note: the folly of this approach is highlighted by a trial which found removing on average 2.8 non-essential drugs from the elderly at one facility caused their 1 year death rate to go from 45%-21% and their hospitalizations that year to go from 30%-11.8%. As far as I know, there is no intervention on the market which offers a benefit comparable to this.
Radiographic Screenings
One of the common ways mass screenings are done is through giving lots of patients X-rays and then funneling those with abnormal imaging into being treated.
For example, women over the age of 50 are advised to get a mammogram every two years so that their deadly breast cancers can be identified and the women can be saved through early treatment for the cancers. However, whenever these screening programs are studied, they are found to not provide a net benefit because:
•Fast growing cancers (the ones you want to catch) will rarely be in the early stage at the exact same time someone gets a mammogram. Conversely, these cancers are normally noticed by doctors or patients (due to the sudden changes they create) and hence are radiographically evaluated independently of the mass screening programs.
•Slow growing cancers (which are unlikely to endanger women) are typically the ones which get caught.
•False positives are quite common with mammograms.
•A positive mammogram result is extremely psychologically stressful and frequently results in a variety of harmful treatments being performed on the women (e.g., having their breasts removed).
Peter Gøtzsche in turn conducted an exhaustive review of the evidence on routine mammogram screening which should have ended the practice (it can be read here). However, his data (which was widely publicized) had no effect on these screening programs. Many (myself included) believe that was because radiologists make so much money from mammograms they have an inherent need to justify the necessity of this routine screening.
Note: many medical specialists depend upon repeatedly performing the same billable service (e.g., vaccinating a child, performing a female pelvic exam, or reading a mammogram).
DEXA Scams
Another universal screening practice for women are dual energy X-ray absorptiometry (DEXA) scans, which calculate the density of bones and hence are believed to be a proxy for bone strength. It is then compared to the average bone density of a 30 year old, and a statistical method is applied to determine how far away their density is from that value which then produces their T-score. Every medical student in turn is taught that a T-score of 0 to -1 is normal, -1 to -2.5 is on the way to being bad (osteopenia) and a T-score that is -2.5 or worse means your bones are weak enough that you have osteoporosis and must urgently begin treatment for it.
If you take a step back, a few questions should come to mind.
First, since bones naturally become less dense with age, most people will have bones that are less dense than those of a 30 year old. In turn, the current of management of osteoporosis accepts that bone loss is inevitable and reasonably tries to prevent that loss early on since it is so much harder to regain it later in life.
Hence, many people due to the normal process of aging will have osteopenia or osteoporosis. Consider for example what this study concluded was the average T-score by age of Italians.
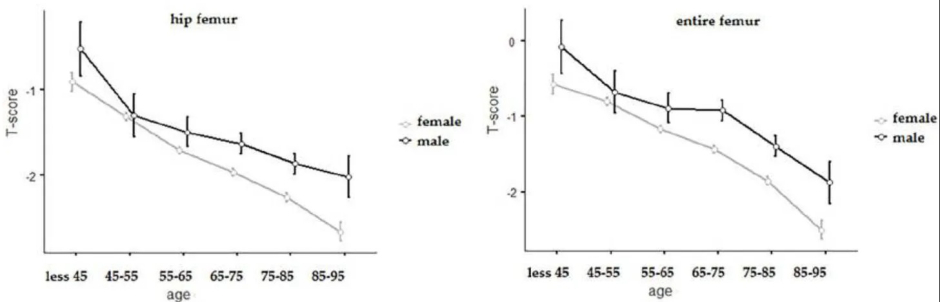
Note: if, for instance, the average T-score for a group is -2.5, this will mean a lot of people within that group (half of them) will have a score below -2.5 and conversely, at lower "averages" even more will have osteoporosis. Additionally, T-scores are calculated utilizing the standard deviation of the bone densities in 30 year olds, a value which can be up to 50% smaller than that of older adults (making it much easier to pass the -2.5 threshold).
Second, how accurate are the scans? As it turns out, there is actually a great deal of variance in DEXA scan results depending on which machine is used, how the operator performs the test and what bones are measured, with studies often finding a 5-6% difference in bone density depending on where the test was done. More importantly, since the T-score is based off standard deviations, a 5-6% difference in bone density can, in turn, change the T-score by 0.2-0.4 (which equates to a decade of bone loss) and hence tip many over to an osteoporosis diagnosis.
Note: a similar issue exists with blood pressure, as the stress of being a doctors office often creates enough of a BP elevation for people to be erroneously diagnosed with hypertension and started on blood pressure medications. This condition, in turn, is euphemistically known as "white coat hypertension," applies to 15-30% of hypertension diagnoses, but rarely is corrected.
Third, is there any point to repeatedly doing them? As it turns out, a study of 4124 older women found that once an initial DEXA result was obtained, there was no additional information of use gained from repeating the study over the next 8 years. Nonetheless, many guidelines often recommend getting a scan every 1-2 years, and likewise, Medicare pays for one every 2 years. As these scans typically cost between $150 to $300, that quickly adds up.
Fourth, do the scans accurately reflect bone strength and the risk of fractures? While they are generally predictive of the risk, they are not as accurate as is commonly believed. For example, this study found the osteoporosis status of a patient (determined by their T-score) frequently did not match what was directly observed within bones under a microscope. Similarly, this study found that when bones were deliberately weakened, Dexa scans underestimated how much strength had been lost.
Note: a cheaper method of diagnosing bone strength (which does not expose patients to ionizing radiation) is beginning to be used in Europe. It works by sending ultrasound waves into bone and then analyzing the spectrum created by those waves to assess the health of the bones. As the attached presentation shows, it accurately predicts bone density, and additionally, predicts bone strength. In short, this may be a dramatically superior approach to Dexa scans, but it is unlikely we will see it enter regular use in the United States for at least a decade due to how heavily invested many already are in performing Dexa scans.
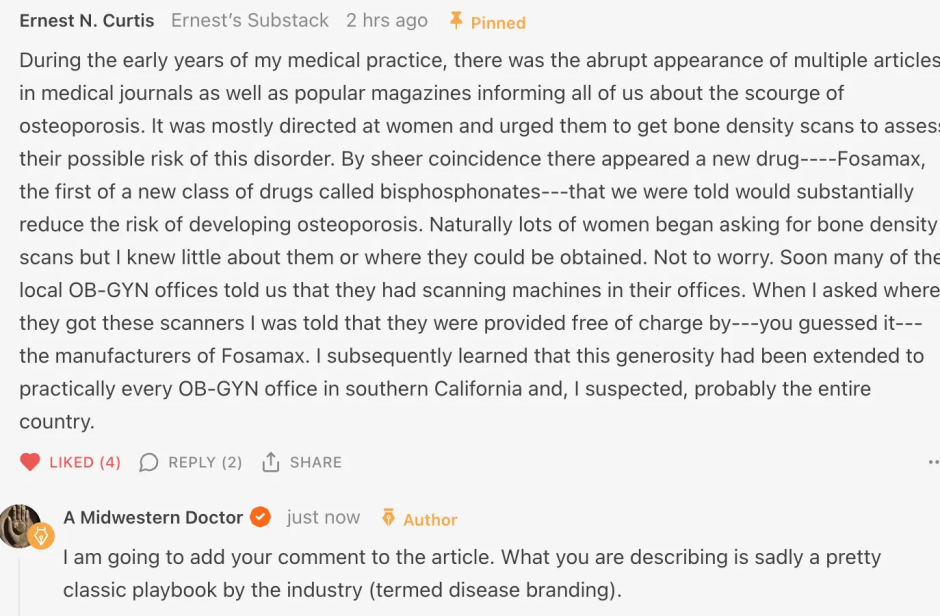
Note: the story above in the comment is discussed in more detail in this NPR article. Additionally, after publishing this article, I learned that of a 2011 book that exposed the DEXA scam and provides many more compelling references arguing against their diagnosis.
Bisphosphonates
Once a patient is diagnosed with osteoporosis (and in some cases after an osteopenia diagnosis), the first line treatment is to start a bisphosphonate and continue it for up to 3-5 years depending on if the drug is administered intravenously or orally.
Note: the bisphosphonates include: Alendronate (Fosamax), Risedronate (Actonel), Ibandronate (Boniva), Zoledronic Acid (Reclast), Zoledronate (Zometa, Aclasta) Pamidronate (Aredia) Etidronate (Didronel), Neridronate (Nerixia), Tiludronate (Skelid), Clodronate (Bonefos, Loron)
A variety of factors influence the development of bone. Two of the most important ones are the cells that build bone up (osteoblasts) and the cells that break bone down (osteoclasts). Bisphosphonates in turn concentrate in the bone and work by disabling or killing osteoclasts. This thus leads to bone density increasing because the balance of bone production shifts towards building them up rather than breaking them down.
Unfortunately, there are two problems with this approach.
1. Bisphosphonates are notorious for having a large number of side effects. Commonly recognized ones include:
- Irritating the stomach and inflaming or eroding the esophagus (which can sometimes lead to esophageal cancer). This side effect is common enough that it leads many patients to not want to continue the drugs.
- Severe bone, muscle and joint pain throughout the body.
- Osteonecrosis (death of bone tissue) within the jaw. Since so many people have been affected by this (e.g., Kaiser found 0.1% of users were affected), class action lawsuits have been filed against the manufacturers for this debilitating illness ( which revealed Merck's private discussions about it). This appears to be a result of bisphosphonates concentrating in the jaw reducing the jaw's ability to repair itself by around 90%. Remarkably, the American Dental Association even cautions its members to avoid working on patients who are taking a bisphosphonate (presumably due to the liability created by their increased risk of harm from a dental surgery).
- Triggering flu like symptoms when injected.
- Occasionally causing unusual fractures in the hips.
- Roughly doubling one's risk for atrial fibrillation
- Low blood calcium levels (hypocalcemia can often be quite problematic).
- Fatigue, nausea and lack of strength.
- Declining kidney function.
- Inflammation of the eyes.
- Poor healing of bones after fractures.
- Increased risk of fractures
- Note: this is an understandably controversial side effect fraught with conflicting evidence, given that its the opposite of what the drug is supposed to do, but there is now enough evidence that it is acknowledged these drugs increase the risk of certain types of fractures.
To illustrate, a January 2008 FDA alert, warned physicians that all bisphosphonates may cause:
severe and sometimes incapacitating bone, joint, and/or muscle (musculoskeletal) pain... [which] may occur within days, months, or years after starting the medication, and in some patients, may not resolve even after discontinuing the medicine.
Note: we also find a variety of other significant issues occur. For example, we've seen many patients on bisphosphonates develop bone spurs in the jaw (which can be quite challenging for them to deal with). Similarly, a study of individuals who have had fractures after 3-8 years of bisphosphonate usage discovered that they had almost no new bone formation occurring.
2. The way bisphosphonates work is very different to how the body was designed to build healthy bone, and in effect, much of the bone they leave you with is "old bone."
Note: a variety of other newer drugs exist to treat osteoporosis. These drugs are often more effective at producing stronger bones, and often don't have the same significant side effects seen with the bisphosphonates, so quite a few of my colleagues use them. Unfortunately, those drugs tend to be much more expensive and each one still has its own set of side effects.

Physiologic Momentum
One of the most remarkable aspects of the human body is its ability to gradually adapt to whatever circumstances it finds itself in. Conversely, one of the primary challenges one faces when dealing with a chronic illness is that typically by the time the symptoms of the disease emerge, the maladaptive physiologic process that gave rise to those symptoms is firmly established within the body and hence quite difficult (and time consuming) to shift.
For example, Alzheimer's disease typically is a result of the processes which create neurons slowing down and being outpaced by the processes that destroy them, hence leading to an increasing neuronal loss and an increasing loss of neurological function. In turn, the only method which has ever been proven to treat Alzheimer's is to simply reverse that equation and have neuronal production outpace neuronal destruction. Unfortunately, since a drug can't be made to do that (rather it requires changing one's lifestyle) the industry has instead relentlessly focused on drugs which eliminate the plaque the brain forms to protect its neurons from injury. Thus all we have to show after decades of spending billions each year to find a cure for this disease are expensive plaque targeting that have a wide range of side effects and are useless for actually treating Alzheimer's disease.
One of the most important adaptive processes in the body is how it accommodates to the stresses and loads placed upon it. For example, the reason why weight training "works" is because muscles being stressed through overexertion gives a signal to the body that it needs to build more muscle.
However, while the adaptive process with muscles is frequently recognized, many others are not. For instance, the body continually remodels the soft tissue which connects the body together, and as a result, when someone experiences a pharmaceutical injury which damages the body's ability to rebuild those tissues, they are likely to subsequently experience a critical structural failure.
This is most well known with the fluoroquinolone antibiotics, as the drugs (which have a high degree of toxicity to the mitochondria that fuel tissue buildup in the body) frequently cause tendon ruptures to occur over a month after the drugs are stopped. Similarly, we also observe many of the other more dangerous drugs on the market over time (even if stopped) will cause the soft tissue of the body to become compromised (often to a degree which significantly impacts the patient's life), which in part may be explained by the fact the cells that create connective tissue have abundant mitochondria.
Note: a more detailed discussion of the treatments for ligamentous laxity (hypermobility is a condition that disproportionately affects the individuals who are the most sensitive to their environment and being injured by pharmaceuticals) can be found here.
Bone Remodeling
An adaptive process also continually reshapes the bones so that their architecture is arranged to optimally bear the loads placed upon them. In most cases, we never think about this process because it just works as intended. However, in certain cases, we do recognize where it has gone awry.
For example, since the bones depend upon the weight of gravity for the signal to be built up ( via the electrical currents that are created when bone is compressed), that signal is lost in low gravity environments. Because of this, a longstanding problem in space travel was the rapid bone loss astronauts experienced (e.g., in 6 months they lost 6-10% of their bone density, which put them at a high risk for fractures once they returned to normal gravity and typically took 3 or more years to recover from).
Because of this, while we typically only focus on the cells which build bone, the reality is that the osteoclasts are also immensely important, as their destruction of bone is what allows bone to assume the shape which best allows it to effectively bare the weight of gravity. In turn, when they are blocked by a bisphosonate, bone density increases, but the bones that form are much more brittle and inflexible. Our dislike of those drugs in turn comes about from how frequently we encounter the pathologic changes they create in our patient's bones (e.g., we find that while compressive strength may be increased, bone mobility is not, and that is often far more consequential for the patients).
This in turn highlights a common problem in medicine. Frequently doctors are trained to focus on treating numbers (e.g., reducing a "high" cholesterol) under the belief that correcting those numbers creates health. Much of this comes from the fact it's much easier to conduct a study that assesses benefit through the change of a value which is assumed to be good (e.g., a vaccine creating the target antibodies) than it is to evaluate if an actual improvement occurs for patients (e.g., a decrease in the total number of people who died-which in Pfizer's studies did not occur despite the fact "lifesaving" antibodies were consistently being produced).
In short I would argue that while bisphonates may be effective at improving a DEXA score, they aren't necessarily good at improving health.
What Causes Osteoporosis?
Since bone metabolism is linked to many other processes in the body, a variety of things can affect it. In turn, I find that colleagues who focus on treating a specific aspect of the body are often able to provide proof their area of focus is the primary determinant of bone health. This hence makes it quite challenging to establish which area is in fact matters most. That said, there are a few factors of particular importance.
1. Mobility—since bone growth depends upon the signals generated from loading weight on the body, a good case can be made that our increasingly sedentary lifestyles are responsible for the continual increase in osteoporosis occurring in America (e.g., one study found sedentary postmenopausal women lost 2.26% of their bone mass in a year, while those who did a weight training program instead had a 1.17% increase). Additionally, sunlight exposure has been shown to increase bone density (along with providing many other critical health benefits), which further illustrates how problematic being sedentary inside can be.
Note: the contribution of immobility to osteoporosis also touches upon another challenging aspect of chronic diseases—often there is a self perpetuating downwards spiral since many of the causes worsen the others (e.g., osteoporosis increases immobility, poor circulation [which is commonly seen in chronic disease states] also creates immobility and immobility simultaneously impairs fluid circulation).
2. Hormones— in a previous article, I discussed the severe dangers of drugs like Lupron which work by disabling the body's production of sex hormones. One of the most common side effects observed from them is a significant weakening of the bones, which commonly leads those injured by the drugs to remark that they "have bones like an 80 year old" (e.g., you will hear reports of a 30-year-old leaning against a wall with their arm and that bone snapping or them learning they need to get dentures). Furthermore, in many cases these effects are often delayed, which again illustrates how a disruption of the remodeling of bone can ripple out far into the future.
Note: we have also seen cases where patients were prescribed high levels of aromatase inhibitors (drugs which prevent the conversion of testosterone to estrogen) which then appeared to trigger bone loss.
This in turn argues that hormones play a vital role in bone health, and in turn, the hormonal medicine field frequently prescribes estrogen to older women to compensate for the loss of estrogen which accompanies menopause, partly under the belief that hormonal supplementation can hence prevent menopause.
However, while supplemental estrogen appears to help prevent bone loss, we don't focus on this approach because:
•Excessive and unbalanced estrogen frequently causes cancers. While this is a contentious topic in the hormonal medicine field (e.g., many doctors who prescribe hormones insist any link between estrogen and cancer is hogwash), we have personally seen numerous cases where a patient was started on estrogen and then developed a severe cancer—especially if they were given too high of a dose. As such, in cases where we feel estrogen is necessary we take multiple precautions to do it in the safest manner possible.
•In our experience, the most important thing is not the bone's density, but rather its elasticity and mobility. When healthy bones are subject to a loading stress, they bend to accommodate that stress and then spring back into their original shape, whereas if a bone is brittle, once it begins to bend, it will break.
The primary hormone which imparts elasticity to the bones (and induces osteoblast activity) is progesterone, and like estrogen, it declines with age—particularly after menopause. In turn, we find that appropriately supplementing progesterone (which unlike estrogen is almost never dangerous), is highly effective at preventing fractures within the body.
Note: osteoporosis, while rarer, also occurs in men. We find that for men, increasing testosterone levels can also help with bone loss, however the magnitude of benefit is not as much as is seen with other hormonal interventions.
3. Inflammation—many of us have observed that patients with chronic inflammatory diseases tend to be at a greater risk of osteoporosis. In turn, the mechanism to support these observations exists as the cytokines classically associated with those inflammatory disease states (e.g., TNF-α and IL-6) have been shown to activate key receptors (e.g., RANKL) which cause osteoclasts to dismantle bone until the underlying disease which is generating those cytokines is addressed.
4. Minerals—since bones are composed of minerals, this suggests bone strength is dependent upon the dietary intake of minerals. Our own experience has been that supplementing with the correct minerals is often what restores bone health, so I am inclined to believe this is indeed a critical point.
Since mineral deficiencies appear to be such a common issue, we've tried to identify what may be responsible for this. Presently we believe the chief culprits are:
•A stomach acid deficiency (since stomach acid is often necessary to absorb dietary minerals). Two of the most common causes of this are acid blocking medications ( which have been repeatedly shown to cause osteoporosis) and the tendency for stomach acid to decline with age (which may in turn explain why osteoporosis increases with age).
Note: a more detailed discussion on the critical importance of stomach acid (e.g., a stomach acid deficiency is one of the most common causes of acid reflux and of autoimmunity) can be found here.
•The chronic depletion of essential micronutrients and minerals from the soil due to industrial agricultural practices (it's a huge problem) and the removal of the mineral rich components of food when they are processed (e.g., when changing a whole grain into a refined grain).
•The tendency for the widely used herbicide Roundup to behave as a chelating agent which binds essential minerals in the soil (particularly the +2 cations like magnesium) and hence prevents them from entering our bodies.
5. Water Fluoridation—Fluoride was originally added to the water supply because it was a toxic waste product numerous industries needed a liability free way to dispose of. Since fluoride was known to increase bone density, this was used to argue that it could protect our teeth, and hence that it could instead be viewed as a vital nutrient. These attempts were initially unsuccessful (as fluoride has a wide range of toxicities), but eventually, since fluoride was needed to produce the original atomic bombs, for national security reasons, the government relented and added fluoride to the water supply.
Unfortunately, like the bisphosphonates, while fluoride increases bone density, the bone that forms is less healthy and able to function normally. In addition to many of my colleagues believing they've observed this harm within their patients, this has also been demonstrated both by numerous studies linking fluoride to osteomalacia (a condition where the bones soften and hence are more likely to fracture) and by numerous studies finding that administering fluoride increases rather than decreased one's fracture risk. Conversely however, since osteoporosis is defined not by fracture risk but rather by the loss of bone density, I don't feel fluoride (which increases bone density) could be the primary culprit for the increasing osteoporosis rates.
Note: some of the newer research shows that fluoride decreases rather than increases bone density.
6. Pharmaceutical Drugs—In addition to the hormone blockers (e.g., Lupron) and the stomach acid blockers (e.g., Prilosec) other pharmaceuticals have also been shown to significantly increase the risk of osteoporosis, particularly the glucorticoid steroids like prednisone (the vast dangers of which are discussed here). To illustrate—taking them doubles one's risk of a fracture (and even more so for a vertebrae), at typical doses they cause a 5-15% loss of bone each year, and in long term users, 37% experience vertebral fractures (additionally, high dose steroid use increases the risk of vertebral fractures fivefold). Glucorticoid bone loss in fact is such a common problem that treating it is one of the few official indications the FDA provides for bisphosphonates.
Note: other drugs are also known to compromise bones. Opioids for instance have been show to delay the healing of fractures or spinal fusions and when used chronically, to lower bone density and increase the risk of a fracture by 4.13 times,. Some of the other drugs which have also been show to weaken bones include the thiazondones (which are used for diabetes), SSRI antidepressants, the anticonvulsants (which were initially developed to treat epilepsy but are now used for many other conditions), Depo-Provera, and the previously mentioned aromatase inhibitors.
7. Environmental Toxins—as the following links show, variety of widely pervasive environmental toxins (e.g., organophosphates, Bisphenol A, aluminum, cadmium and nicotine, lead, mercury, triclosans, along with many other persistent organic pollutants) can inhibit bone formation and are linked to osteoporosis.
Note: drinking soda has been shown to significantly increases one's risk of osteoporosis and fractures.
At the same time however, I'm not completely sure these points paint the full picture because the most ancient medical texts in the world also discussed osteoporosis (at a time when, for instance, Roundup and Acid Blockers did not exist)
In addition to these mechanisms, there are a few others I suspect cause osteoporosis but I have less evidence to support those claims. In the final part of this article, I will list those mechanisms and our preferred protocols for treating osteoporosis (some of which, such as the minerals are quite simple, others like hormonal management are a bit complicated, along with some that are a more out of the box or that can be done in your younger years to head off a critical loss of bone mass in the future).