By A Midwestern Doctor
The Forgotten Side of Medicine
August 25, 2025
Yale's medical school is widely considered to have one of the top autoimmunity research and treatment programs in America. As long COVID is considered to be immunological in nature, their researchers extensively studied it, and remarkably some of them then pivoted to also studying vaccine injuries (in part because the COVID vaccines rather than curing long COVID patients, sometimes made them much worse). A few days ago, they finished a new research paper on the subject, but like their previous ones, it was immediately summarily rejected by the "reputable" journals it was submitted to (including the one I feel was the most obligated to publish these findings). In this article, I aim to cover the importance of their most recent results and, more important, examine what their habitual censorship reveals about science in general.
Yale's LISTEN Study
All of this research was conducted within Yale's LISTEN Study (Listen to Immune, Symptom and Treatment Experiences Now) where a group of patients with both long COVID and then COVID vaccine injuries were extensively followed, evaluated (e.g., for symptoms and biomarkers) then analyzed to develop a consistent clinical picture of the diseases. As this is an extremely important study. I've been in touch with participants throughout the study, who've shared data consistent with our observations of vaccine-injured patients over the last four years.
Initially, in 2023, they shared some of their preliminary data as a November 2023 preprint (which has still not been accepted for publication) which detailed the common symptoms seen in the 241 participants with post vaccination syndrome (PVS), which match what we've seen in clinical practice:
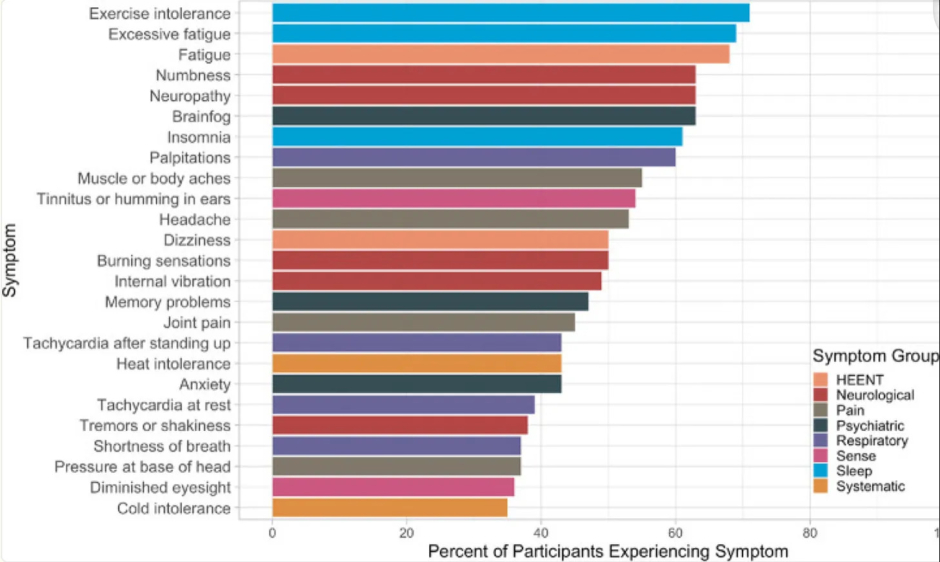
To quote the study:
In conclusion, people reporting PVS after covid-19 vaccination in this study are highly symptomatic, have poor health status, and have tried many treatment strategies without success. As PVS is associated with considerable suffering, there is an urgent need to understand its mechanism to provide prevention, diagnosis, and treatment strategies.
Note: these results were discussed in more detail in this October 2023 online conference (e.g., the mast cell component of the illness). From watching this conference, my impression was that the investigators sincerely want to help the trial participants, but due to the unpleasant implications of their findings, are in a very challenging position (hence why their 2023 pre-print has still not been published).
In February 2025, they published a much more detailed study, that unfortunately also remains a preprint (as no journal would publish it). It was comprised of 42 post-vaccine syndrome (vaccine-injured) participants (and 22 controls) and detected a variety of concerning changes. These included lower CD4 cells and elevated TNFα+ and CD8 T cells (which equates to a picture of immune suppression and autoimmunity). Additionally, post-vaccine syndrome (PVS) participants had a tendency for the re-activation of chronic infections and had a chronic persistence of the spike protein. The more detailed data was as follows:
General Health
Vaccine-injured individuals reported lower general health scores, such as lower physical function scores, higher anxiety, depression, fatigue, and pain scores and increased sleep disturbances.
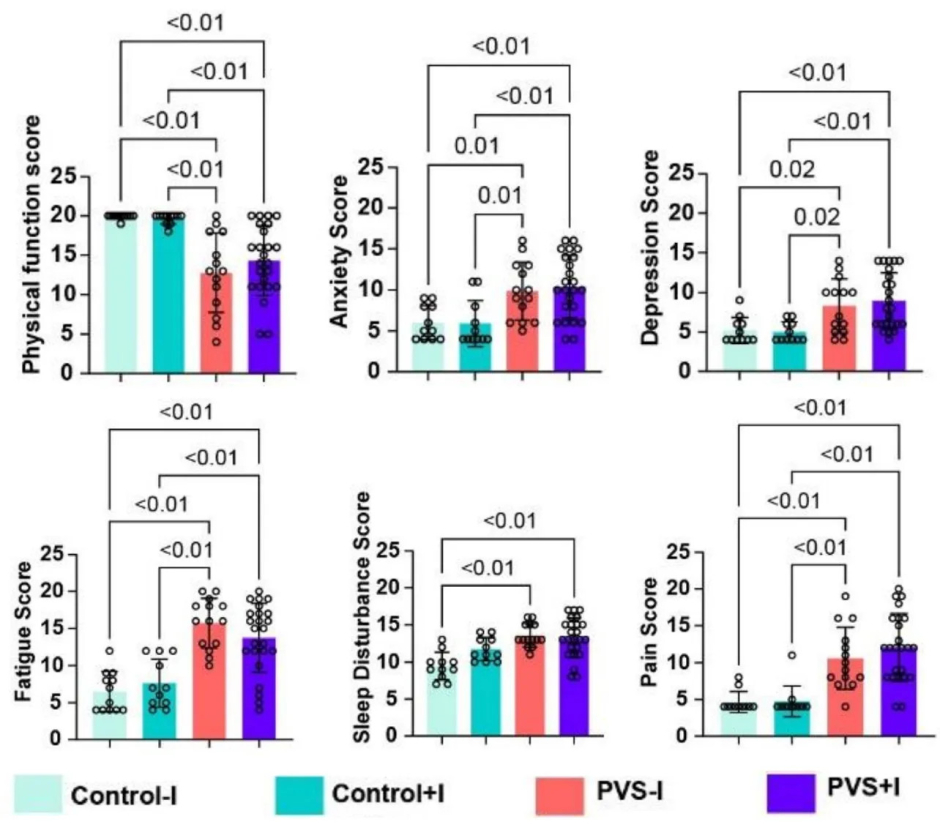
This is important because it demonstrates that vaccine injuries are a real condition with actual health effects (rather than just 'being in your head').
Spike Protein Persistence
To my knowledge, their second study provides the best demonstration that the COVID vaccine persists for a prolonged period within the body and when present, typically is much higher than in controls.
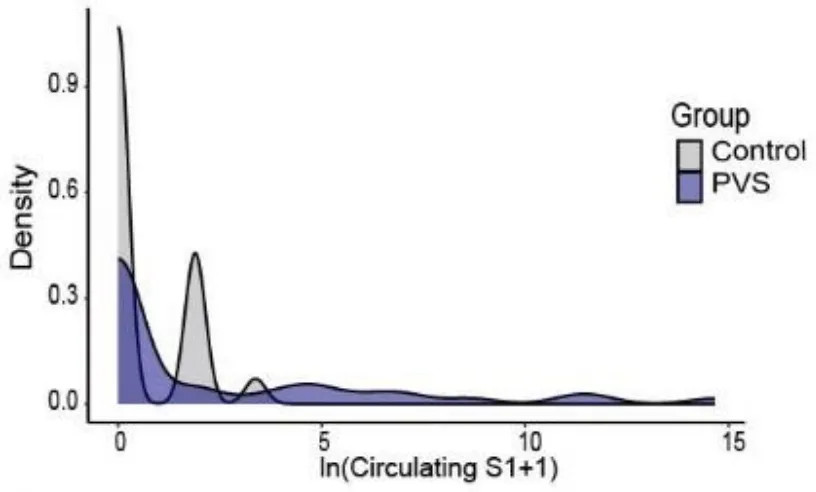
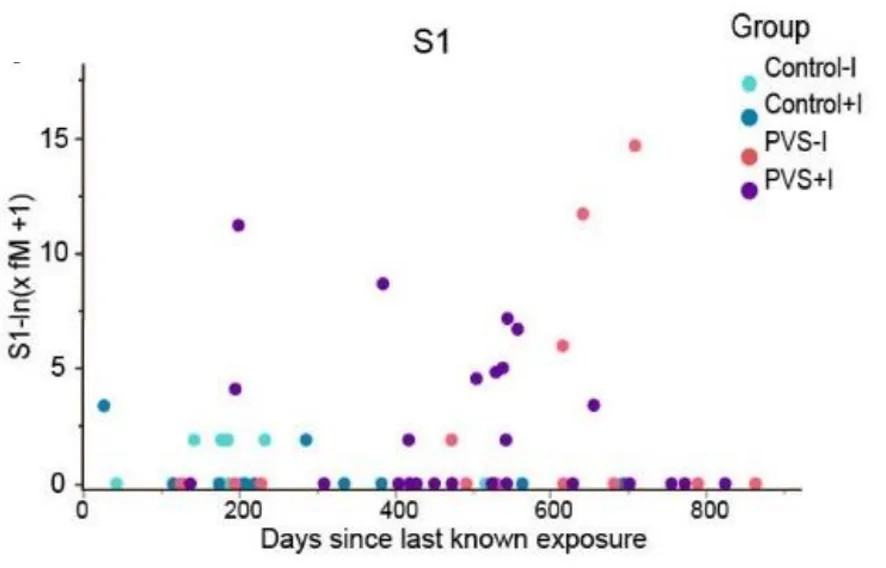
Total spike protein present in each participant at final evaluation
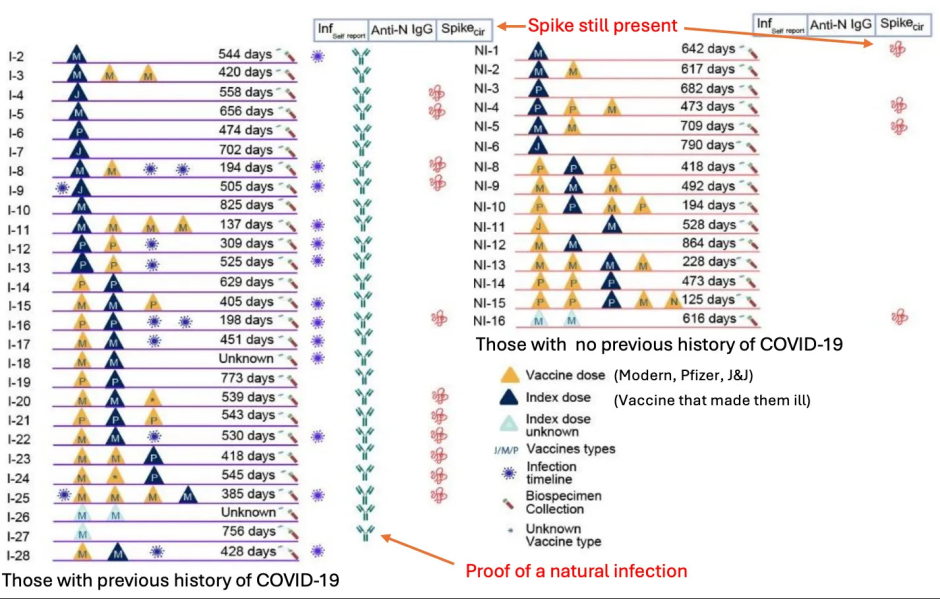
This data collectively shows that:
• The COVID vaccine spike protein can persist for years in the body. The major limitation with each previous study was that spike was still found at the end of the study duration, so it was not possible to know how long it actually persisted. As this study shows, a few months was not long enough to measure the spike protein's persistence, as in some cases, it lasted for close to two years (and were it to be measured again, might last even longer).
• In many cases, COVID spike protein persistence eventually stopped but symptoms continued. Assuming this is correct, that means in many cases the vaccine will eventually be eliminated (which may depend upon the vaccine lot they received), and that not all of the post-vaccine symptoms are a result of persistent spike protein production.
• The persistence of the spike protein without any proof of a natural infection provides strong evidence the vaccine's spike protein is what's persisting in the body.
Note: numerous other studies (discussed here), the earliest of which was a March 2022 one by Stanford, have also shown the COVID vaccine persists in the body. While this persistence is typically attributed to the vaccine mRNA integrating with the host's DNA (which does happen), leading to perpetual mRNA production, both I and Dr. Malone (a leading expert in this area) believe the primary (and far more probable) source of persistence was the mRNA being modified to resist degradation (leading to the vaccine mRNA indefinitely producing synthetic spike protein in the body).
This, in turn, was a result of needing to ensure the vaccine persisted long enough to produce sufficient spike protein to produce a vaccine immune response (and hence win an approval) but this being incredibly challenging to do (especially given the rushed nature of Operation Warp Speed and how many companies were racing to get the initial approval and the billions in profit that would follow). Consequently, developers prioritized maximizing the mRNA vaccine's persistence and productivity, given its unpredictable behavior in the body and to accept that the injuries which followed from excessive spike production within the body were an acceptable price to pay for expediting the vaccine (hence illustrating why blanket liability shields, such as the ones given during Operation Warp Speed, are so problematic).
Immunologic Suppression and Viral Reactivation
One of the major problems with the COVID vaccine has been that it causes a significant number of people to develop signs of immune suppression, such as frequent flu infections or reactivation of chronic viral infections (e.g., shingles in general along with severe cases of shingles has been strongly linked to vaccination).
Note: less severe versions of this immune suppression have also been observed to follow shedding exposures.
A variety of theories have been put forward to explain why this happens, such as:
• The immune system being locked onto the vaccine antigen, which results in it losing the ability to target other natural antigens (and has been proven to be an issue with many other vaccines as well).
• The vaccine creating an IgG4 class switch, which essentially causes the immune system to no longer fight back against COVID spike proteins.
• The overstimulation of the vaccine over time causes a suppression of spike protein antibodies (which the study observed). This could either be a result of the vaccine-injured patients have an existing inability to develop immunity to the vaccine's spike protein (as suggested by the January 2023 study) or that the vaccine gradually eliminated the body's ability to bind to the spike protein, resulting in individuals becoming more vulnerable to the spike protein over time if they happened to have a long-acting vaccine continue to produce spike protein inside them.
• The spike protein collapsing the body's zeta potential (which as it gets more severe can cause blood clots of increasing sizes). Since many symptoms of infectious illnesses result from the zeta potential collapse they create, those symptoms of illness are magnified when there is already an impaired zeta potential (which the spike protein has been shown to collapse).
• The spike protein directly destroying immune cells (e.g., CD4 cells-something also seen in HIV) and the stem cells that create the immune cells.
Note: these labs were sent to me by one vaccine-injured participant in the study.
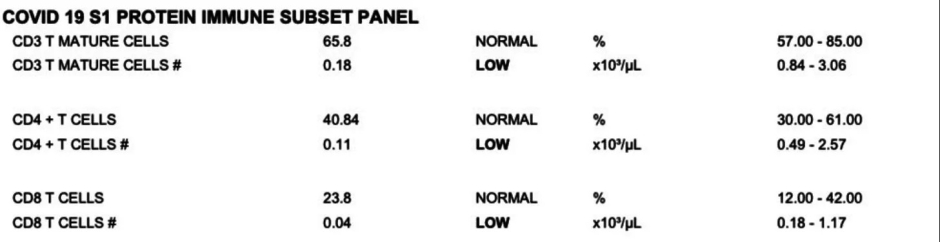
In addition to showing a loss of key immune cells, the study also showed both the CD4 and CD8 cells had signs of being "exhausted," as changes were observed in them that are known to correlate with those cells partially losing ability to respond to infections due to a chronic over-activation of them (e.g., by persistent vaccine spike protein).
Finally, much in the same way that there were signs of immune dysfunction, the study also observed consistent significant signs of viral reactivations in the cohort, most notably with Epstein Barr virus, but also with herpes and frequently both concurrently (however for some reason, shingles was not assessed in this study). In turn, we have frequently seen EBV be a component of the vaccine-injury picture (to the point sometimes it needs to be treated) and frequently also observe an increase in herpes.
Note: one of the best treatments I have found for all three of these viruses is ultraviolet blood irradiation (discussed here). Additionally, DMSO can be quite helpful for shingles and herpes (discussed here).
Additionally, there was also a possible increase in seropositivity to a few other pathogens (e.g., H. Pylori and the parasite Toxocara), which could potentially (but more likely than not doesn't) explain some of the gastrointestinal issues seen in vaccine-injured patients or their response to ivermectin.
Autoimmunity
One of the most common issues associated with the COVID vaccines were autoimmune disorders (detailed here) due to the fact the spike protein had an unusually high overlap with human tissue and because it was designed to express itself on the surface of human cells. In this study, Yale's team reported:
We observed significant increases in IgM reactivities against 65 antigens, IgG reactivity against 1 antigen and IgA reactivities against 39 antigens in PVS compared to controls after multiple testing corrections. Among these antigens, two showed log₂fold change of greater than 2: anti-nucleosome IgM [which is strongly associated with lupus] and anti-AQP4 IgA [which is associated with a rare autoimmune disorder that attacks the central nervous system, particularly optic nerve and spinal cord].
Note: a significant increase in TNF⍺ levels in simulated CD8+ cells ( which can often lead to immune dysfunction) and a non-significant increase in CD8+ IFNγ were observed.
I feel these results are important as they validate something many of us have been claiming for four years with the vaccines.
Note: less severe versions of autoimmunity have also been observed to follow shedding exposures.